Courtesy: Prof Nabil Ebraheim, Unviersity of Toledo, Ohio, USA
Jones fracture is a fracture of the base of the fifth metatarsal.
- First described by British surgeon Robert Jones, who sustained the fracture while dancing.
Definition and Location
- Occurs at the metaphyseal–diaphyseal junction of the fifth metatarsal.
- Extends into the intermetatarsal joint between the fourth and fifth metatarsals.
- Located distal to the metatarsocuboid joint.
- Typically occurs ~1–1.5 cm distal to the tuberosity of the fifth metatarsal.
Relevant Anatomy
- Fifth metatarsal has head, neck, shaft, and tuberosity.
- Base of the fifth metatarsal articulates with:
- Cuboid bone metatarsocuboid joint
- Fourth metatarsal intermetatarsal joint
Blood Supply
- Tuberosity region receives blood from multiple metaphyseal arteries.
- A nutrient artery supplies intramedullary branches with retrograde flow.
- Fractures distal to the tuberosity may disrupt the nutrient artery, creating relative avascularity.
- Limited blood supply contributes to delayed healing or nonunion.
Tendon and Soft Tissue Attachments
- Peroneus brevis tendon inserts at the tuberosity of the fifth metatarsal.
- Plantar fascia (lateral band) attaches to the fifth metatarsal.
- Tendon pull can separate fracture fragments and impair healing.
Clinical Considerations
- Fractures may be mistaken for lateral foot or ankle sprains, which are common in this region.
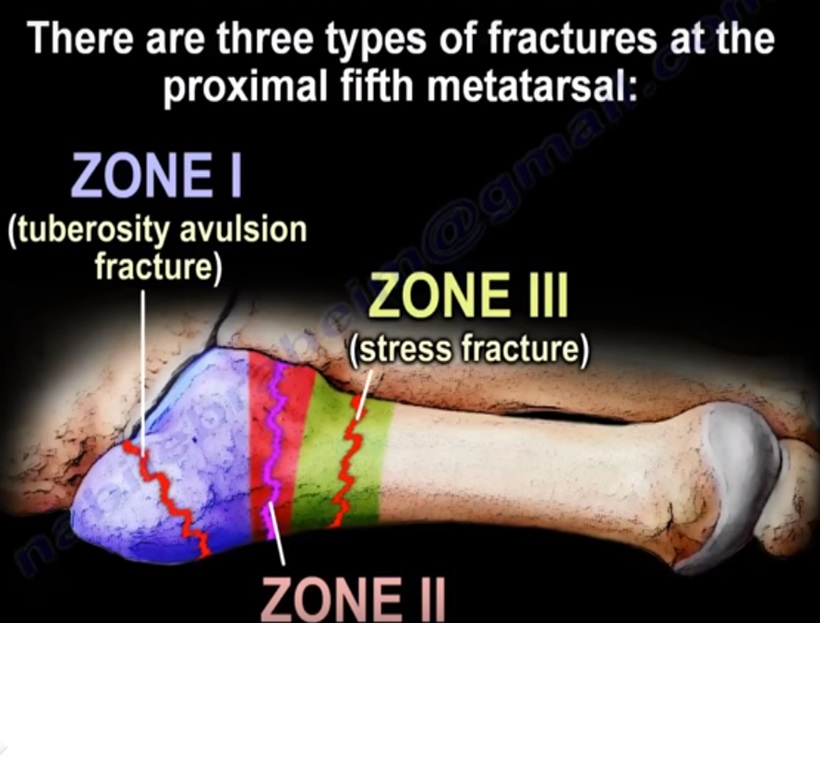
Classification of Proximal Fifth Metatarsal Fractures
- Zone 1 – Avulsion fracture
- Occurs at the tuberosity.
- Also called pseudo-Jones fracture.
- Usually treated conservatively.
- Zone 2 – True Jones fracture
- Occurs at the metaphyseal–diaphyseal junction.
- Involves the articulation between the fourth and fifth metatarsals.
- Higher risk of nonunion due to limited blood supply.
- Zone 3 – Stress fracture
- Occurs distal to the fourth–fifth intermetatarsal articulation.
- Usually chronic stress injuries.
- May be associated with cavovarus foot deformity.
Pediatric Consideration
- Normal apophysis (growth plate) appears between ages 9–14.
- The apophysis runs parallel to the shaft of the fifth metatarsal and can mimic a fracture on imaging.
Imaging Findings
- X-rays confirm fracture and location.
- Acute Jones fracture:
- Sharp fracture margins.
- No medullary sclerosis.
- Stress fracture:
- White fracture line.
- Medullary sclerosis present.
Treatment
- Non-displaced fractures
- Immobilization with boot or cast.
- Non-weight-bearing for 6–8 weeks.
- About 75% heal with conservative treatment.
- Displaced fractures or athletes
- Intramedullary screw fixation commonly performed.
Surgical Considerations
- Fifth metatarsal appears straight on lateral view and curved (lateral bow) on AP view.
- Lateral bow can create surgical complications.
- Risk of medial cortex perforation at the mid-shaft.
- Intramedullary canal is narrower in the plantar–dorsal dimension.
- Entry point for screw or guide wire is not exactly centered due to anatomy and the metatarsocuboid joint.
Screw Fixation Guidelines
- Each metatarsal should be evaluated individually for screw size and placement.
- Screw should be parallel to the shaft in the lateral plane.
- Avoid directing the screw plantarward.
- Avoid injury to the sural nerve.
- Common screw size: 4.5 mm cancellous screw.
- Typical screw length: 40–50 mm.
- Screw diameter depends on intramedullary canal width.
- Small screw – unstable fixation.
- Oversized screw – fracture displacement.
- Screw must cross the fracture site.
Causes of Fixation Failure
- Poor blood supply to the fracture area.
- Premature return to activity before complete radiographic healing.
Leave a Reply