Courtesy: Prof Amr Abdelgawad, Associate Professor, Texas Tech University, USA
- Anatomy
- 5th metatarsal base:
- Insertion of Peroneus brevis tendon
- Common site of avulsion injuries (inversion)
- Blood supply
- Poor at metaphyseal–diaphyseal junction
- Risk of delayed union / non-union
- Growth Plate vs Fracture (X-ray Differentiation)
| Feature | Growth Plate (Apophysis) | Fracture |
| Direction | Parallel to metatarsal | Perpendicular / transverse |
| Age | Appears: ~9 yrs | Any age |
| Closure | Girls: ~12 yrs, Boys: ~14 yrs | — |
| Edges | Smooth | Sharp, irregular |
Key exam point:
If line is parallel – normal apophysis
If transverse – fracture
- Mechanism of Injury
- Inversion injury of foot
- Peroneus brevis pulls avulsion
- Clinical Presentation
- Pain + swelling over lateral foot
- Tenderness at base of 5th metatarsal
- Difficulty weight bearing
Important:
- Pain at base – Foot X-ray (not ankle)
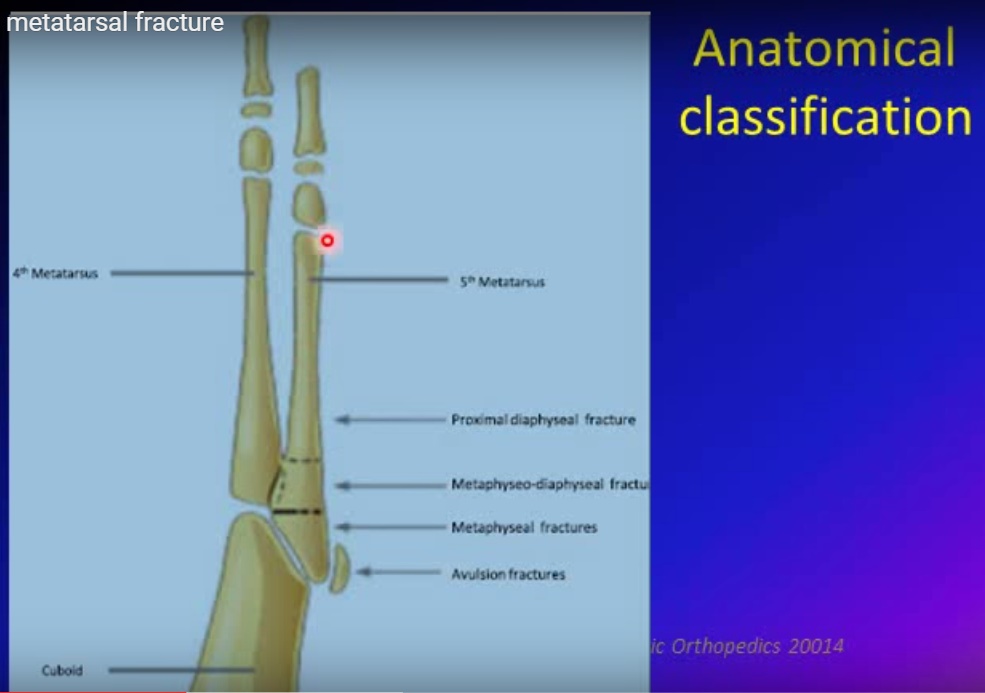
- Anatomical Classification
Fractures based on location:
- Physeal (apophyseal)
- Metaphyseal
- Metaphyseal–diaphyseal junction
- Proximal diaphyseal (stress)
- Types of Fractures (Most Important for Exams)
1. Avulsion Fracture (Pseudo-Jones)
- Location: Tuberosity (metaphysis)
- Mechanism: Peroneus brevis pull
- Stable
Treatment:
- Weight bearing as tolerated
- Hard sole shoe / boot / bandage
- No follow-up X-ray needed
2. Metaphyseal Fracture
- Also stable
Treatment:
- Same as above
- Early weight bearing
3. True Jones Fracture
- Location: Metaphyseal–diaphyseal junction
- (Between 4th & 5th metatarsal articulation)
Important:
- Poor blood supply
- High risk of non-union
Treatment:
- Non-weight bearing cast
- Prolonged immobilization
Athletes:
- Intramedullary screw fixation (early return)
4. Proximal Diaphyseal Stress Fracture
- Seen in:
- Athletes
- Varus foot loading
High risk of non-union
Treatment:
- Often surgical (IM screw)
- Radiological Landmark for Jones Fracture
- If fracture line:
- Toward cuboid Pseudo-Jones (stable)
- Between 4th & 5th MT – True Jones (unstable)
- Orthopedic Referral Indications
- Suspected Jones fracture
- Displacement
- Non-union risk
- Athlete needing early return
- Diagnostic uncertainty
- Key Exam Pearls
- Most common – Pseudo-Jones (avulsion)
- Most dangerous – True Jones fracture
- Growth plate = parallel line
- Fracture = perpendicular line
- Always:
“Pain at base X-ray foot, not ankle”
- Quick Summary Table
| Type | Stability | Blood Supply | Treatment |
| Avulsion (Pseudo-Jones) | Stable | Good | WBAT, boot |
| Metaphyseal | Stable | Good | WBAT |
| Jones | Unstable | Poor | NWB cast / surgery |
| Stress fracture | Unstable | Poor | Surgery often |

Leave a Reply