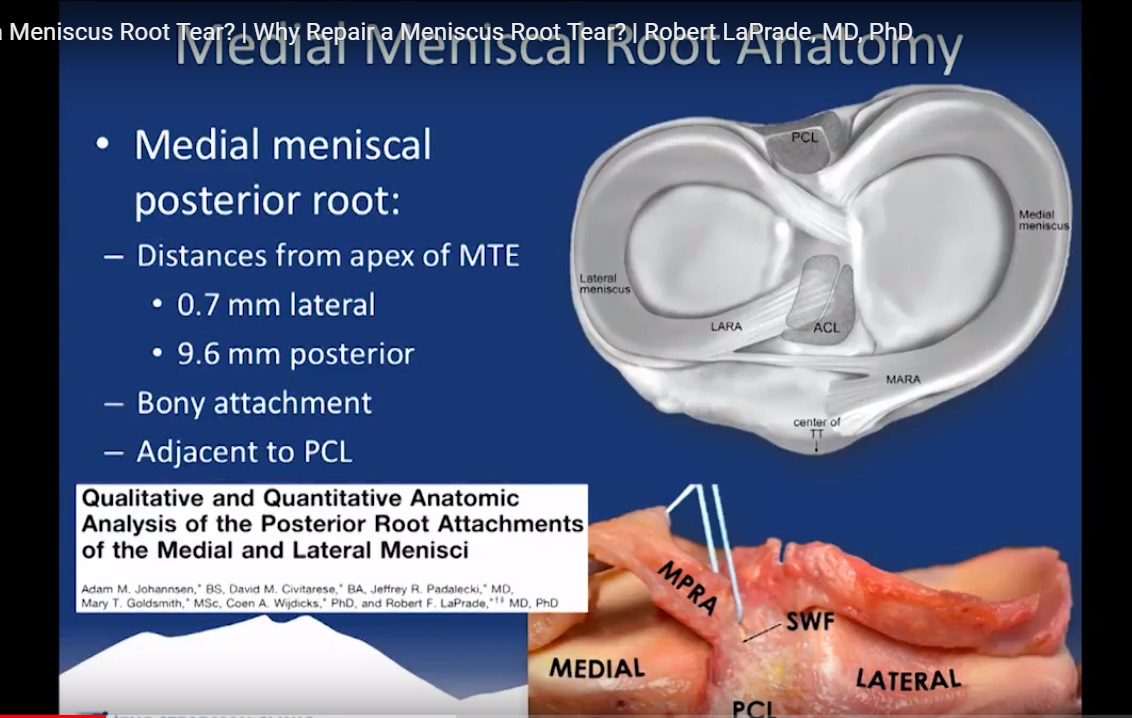
Courtesy: Robert laPrade, Complex Knee Surgeon, Steadman Philippon Research Insitute, Vail, Colarado, USA
Root tears have been described as a silent epidemic. They are not as rare as they were once thought to be. These tears are often missed on an MRI and arthroscopic diagnostics. Theses tears can lead to rapid development for knee osteoarthritis.
Mainly, radial root tears cause knee osteoarthritis. Similar loading characteristics as root tears. Up to 28% of overall meniscal tears in some series. Radial tears near the root attachment can simulate root avulsions both functionally and on imaging.
Why repair a meniscus root tear? The literature has shown that a meniscus root tear is equivalent to a total medial meniscectomy. The medial meniscus repair restores contact pressure to normal. Radial root tears are equivalent to a root tear. Anatomic medial meniscus root repairs restore contact area and minimize peak contact pressures.
The consequences of a non-anatomic root repair does not restore contact pressure or contact area. Implications show that need to release subluxed root tears. Anterior lateral meniscal root tears are intimately associated with ACL tibial insertion. Broad lateral posterior attachments.
Why repair a lateral meniscus root tear? Anatomic lateral meniscus root repairs restore contact area and minimize peak contact pressures. Increased knee AP and rotatory instability due to posterior lateral meniscal root disruption may contribute to increased loads on an ACL reconstruction graft.
Medial meniscus root tears are often associated with chondral injuries and lateral meniscus root tears are often associated with ACL tears. Patients are 10 times more likely to have an ACL tear with a lateral meniscus tear than patients with medial meniscus root tears. Iatrogenic tears have been reported in all four root tears.
Almost all medial and lateral meniscus root tears are type 2: extrusion, bone marrow edema, lower grade cartilage lesions. It is very difficult to test for meniscus root tears in a clinical exam. Patients with a root tear will have deep posterior knee pain with maximum knee flexion. When repairing a meniscus root tear, transtibial pull-out repair is the gold standard.
The literature has shown improved functional outcomes following transtibial pullout repair with a mean follow-up of 30 months. Radiographs also showed no osteoarthritis progression in 84% of patients. MRI showed no osteoarthritis progression in 82% of patients. In conclusion, it is important to not miss a root tear. Age does not matter, but cartilage status does. consider two-tunnel transtibial repair.
This was very informative. How are.meniscal root tears caused and when can a spirts person return to activity after rehab?