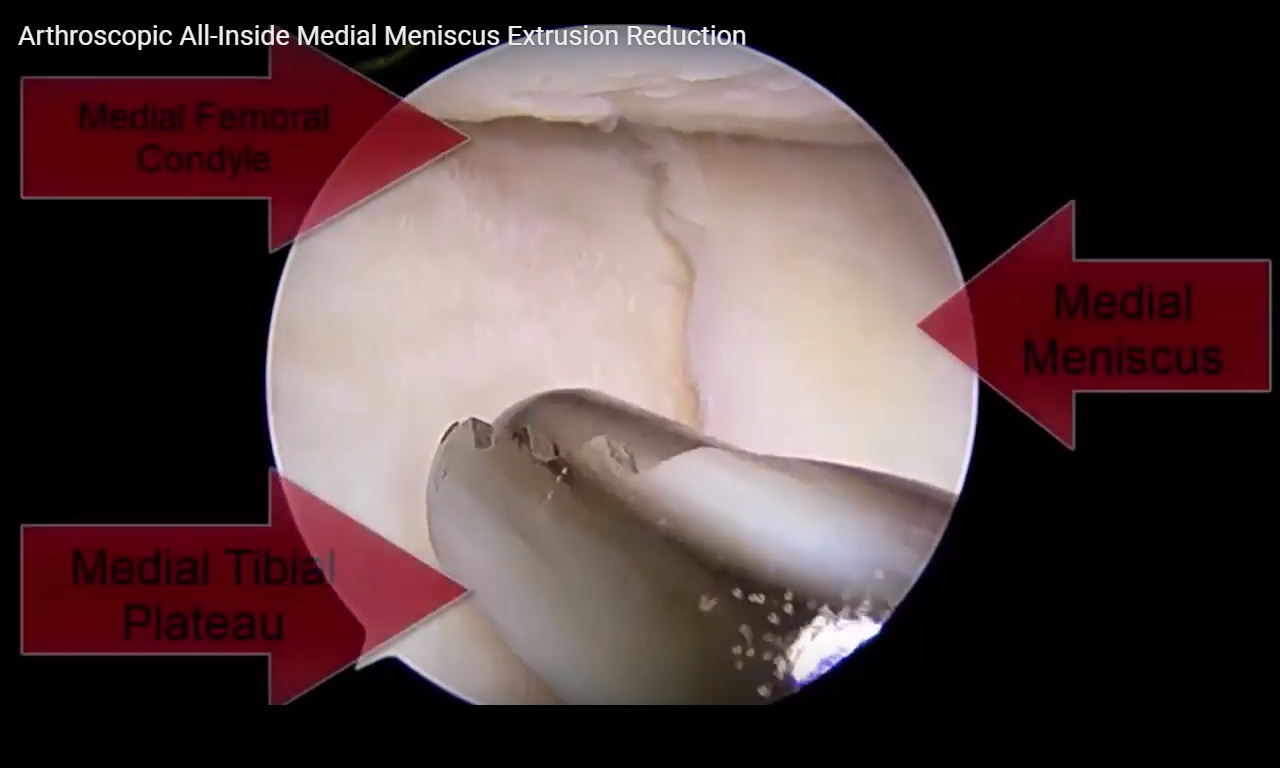
Courtesy: Justin Arner MD, Associate Professor, University of Pittsburgh, Pennsylvania, USA
Meniscus Anatomy and Function
-
The medial meniscus is C-shaped; the lateral meniscus is more U-shaped and mobile.
-
Composed primarily of:
-
Type I collagen (predominantly peripheral)
-
Type II collagen (more central)
-
High water content
-
Glycosaminoglycans
-
-
Functions:
-
Load transmission
-
Shock absorption
-
Stability
-
Lubrication
-
Proprioception
-
Vascular Zones
-
Peripheral “red zone” has vascular supply.
-
Central “white zone” is avascular.
-
Central tears have limited intrinsic healing potential.
-
Peripheral tears demonstrate better fibrocartilaginous healing.
Why Meniscus Preservation Matters
Evidence consistently demonstrates:
-
Reduced long-term osteoarthritis compared with meniscectomy.
-
Improved patient-reported outcomes.
-
Higher reoperation rates compared with partial meniscectomy.
-
Failure rates reported between 16 percent and 29 percent depending on tear type and follow-up duration.
Bucket-handle tears have particularly high reoperation rates, approaching 20 percent or more in some studies.
Repair Techniques
Inside-Out Technique
-
Traditional approach.
-
Requires posterior incision and capsule tying.
-
Considered technically reliable with strong fixation.
All-Inside Technique
-
Faster and technically less demanding.
-
Modern devices improve efficiency.
-
Clinical outcomes similar to inside-out techniques in many studies.
Key Observation
-
Failure rates increase with longer follow-up.
-
Medial meniscus repairs fail more often than lateral.
-
Poor preoperative function and use of allograft in associated anterior cruciate ligament reconstruction may increase failure risk.
Biological Requirements for Healing
Successful meniscus healing requires:
-
Appropriate cell types
-
Adequate cell numbers
-
Extracellular matrix formation
-
Growth factor signaling
-
Controlled inflammatory response
Positive Growth Factors
-
Fibroblast growth factor
-
Platelet-derived growth factor
-
Transforming growth factor beta
Platelet-derived growth factor appears particularly important for:
-
Cell proliferation
-
Matrix production
Negative Factors
-
Tumor necrosis factor alpha
-
Matrix metalloproteinases
-
Excess inflammatory cytokines
Balancing inflammation after injury and surgery is critical but often underappreciated in clinical practice.
Mechanical Methods to Enhance Healing
Rasping
-
Refreshes tear edges.
-
Encourages synovial ingrowth.
-
Simple and inexpensive.
Trephination
-
Creates vascular channels using a needle.
-
Theoretical benefit in improving blood supply.
-
Concerns exist regarding structural weakening.
Bone Marrow Venting (Notch Microfracture)
-
Stimulates marrow elements to enter joint.
-
Mimics biological effect seen during anterior cruciate ligament reconstruction.
-
Some randomized studies show improved healing rates.
-
Simple and cost-effective.
Fibrin Clot Augmentation
-
Provides scaffold with platelets and cytokines.
-
Historically used.
-
Some early studies showed lower failure rates.
-
Technically demanding.
-
Limited modern large-scale data.
Platelet-Rich Plasma
Mechanism
-
Concentrated platelets release growth factors.
-
Promotes fibrocartilage formation.
-
Enhances extracellular matrix production.
-
Stimulates chemotaxis and angiogenesis.
Challenges
-
No standardized definition.
-
Variability in:
-
Leukocyte concentration
-
Platelet concentration
-
Preparation techniques
-
Timing of injection
-
-
Cost varies significantly.
Clinical Evidence
-
Some studies show:
-
Lower failure rates
-
Improved magnetic resonance imaging healing
-
-
Other studies show:
-
No significant difference
-
Possible increased stiffness when combined with anterior cruciate ligament reconstruction
-
Overall, evidence remains mixed but promising.
Bone Marrow Aspirate Concentrate
-
Contains mesenchymal stem cells and growth factors.
-
Animal studies show improved healing, including avascular tears.
-
Limited human clinical data.
-
Higher cost and more invasive.
-
Some database studies show no clear reduction in revision rates.
Scaffolds and Meniscus Wrapping
Emerging options include:
-
Collagen matrix wrapping
-
Synthetic scaffolds
-
Hydrogel systems
-
Extracellular matrix-derived materials
Preclinical studies are promising.
Early clinical data suggest:
-
Acceptable failure rates
-
Good patient-reported outcomes
However:
-
No consensus on ideal material.
-
Cost remains a major limitation.
-
Technical demands are higher.
Repurposing Approved Medications
An innovative concept involves using medications already approved for other indications.
Example: Losartan
-
Traditionally used for hypertension.
-
Inhibits transforming growth factor beta.
-
May reduce fibrosis.
-
Animal studies suggest improved cartilage quality.
-
Potential to enhance biological repair response.
Other agents under investigation:
-
Montelukast
-
Simvastatin
-
Anti-inflammatory modulators
These strategies may offer regulatory advantages in certain healthcare systems.
Key Clinical Questions
Does Technique or Biology Matter More?
-
Proper repair technique is essential.
-
Biological augmentation may be the limiting factor once fixation is optimized.
-
Healing assessment remains challenging:
-
Magnetic resonance imaging is imperfect.
-
Clinical outcomes do not always correlate with structural healing.
-
Timing of Repair
-
Earlier repair likely preferable.
-
Delays of several months may reduce healing potential.
-
No definitive time cutoff established.
If Only One Biological Option Is Chosen
Common practical choices:
-
Bone marrow venting (simple and inexpensive).
-
Platelet-rich plasma (most commonly used augmentation).
-
Selection often depends on cost and availability.
Osteoarthritis and Injectable Trends
In early osteoarthritis:
-
Platelet-rich plasma is increasingly favored over hyaluronic acid in many practices.
-
Often administered in series of three injections.
-
Leukocyte-poor formulations commonly preferred.
-
Bone marrow aspirate concentrate used selectively due to cost.
Use of corticosteroids in younger patients is increasingly questioned.
Current Limitations
-
Lack of standardized preparation methods for biological products.
-
Limited high-quality randomized controlled trials.
-
Cost and insurance coverage barriers.
-
Difficulty objectively measuring meniscus healing.
Future Directions
-
Better translational research between laboratory and clinical practice.
-
Standardized biological protocols.
-
Cost-effective augmentation strategies.
-
Tissue engineering approaches integrating cells and scaffolds.
-
Repurposed medications targeting inflammatory and fibrotic pathways.
Conclusion
-
Meniscus preservation is critical to long-term joint health.
-
Failure rates remain clinically significant.
-
Surgical technique is important but likely not the only determinant of healing.
-
Biological augmentation represents the next frontier.
-
Current options include:
-
Rasping
-
Bone marrow venting
-
Platelet-rich plasma
-
Bone marrow aspirate concentrate
-
Scaffold augmentation
-
-
More high-quality clinical trials are needed.
-
The field is evolving, and significant advancements are expected in the coming decades.

Leave a Reply