Courtesy Dr Dinshaw Pardiwala, Dr Ashok Shyam, Ortho TV
Meniscus Repair: Tips, Tricks, and Surgical Pearls
Introduction
Meniscus preservation has become a major priority in modern knee surgery. Increasing evidence shows that preserving meniscal tissue helps maintain joint biomechanics, reduces cartilage degeneration, and delays osteoarthritis progression.
This discussion focuses on practical aspects of meniscus repair, including:
- Decision-making
- Repair techniques
- Ramp lesions
- Discoid meniscus tears
- Root repairs
- Biological augmentation
- Technical pearls and pitfalls
Principles of Meniscus Repair
Primary Goal
The main objective is:
- Preserve the meniscus whenever possible
Repair should generally be attempted if the tear is considered repairable.
Factors Influencing Decision-Making
The decision to repair depends on:
- Tissue quality
- Chronicity of tear
- Tear reducibility
- Presence of secondary tears
- Associated ligament injuries
- Meniscal vascularity
Case 1: Chronic Locked Bucket-Handle Tear
Clinical Scenario
- 38-year-old female
- Eight-month history of locked knee
- Persistent pain and locking
- MRI showed:
- Locked bucket-handle tear of lateral meniscus
- Intact ACL
- No arthritis
Challenges in Chronic Tears
Chronic tears may develop:
- Meniscal shortening
- Deformation
- Reduced healing potential
Despite this, lateral meniscus preservation remains important.
Surgical Strategy
Step 1: Achieve Reduction
Reduction feasibility is one of the most important determinants of successful repair.
Step 2: Freshen the Tear Edge
Techniques include:
- Shaver
- Meniscal rasp
Goal:
- Create a bleeding vascular surface
Step 3: Initial Reduction Stitch
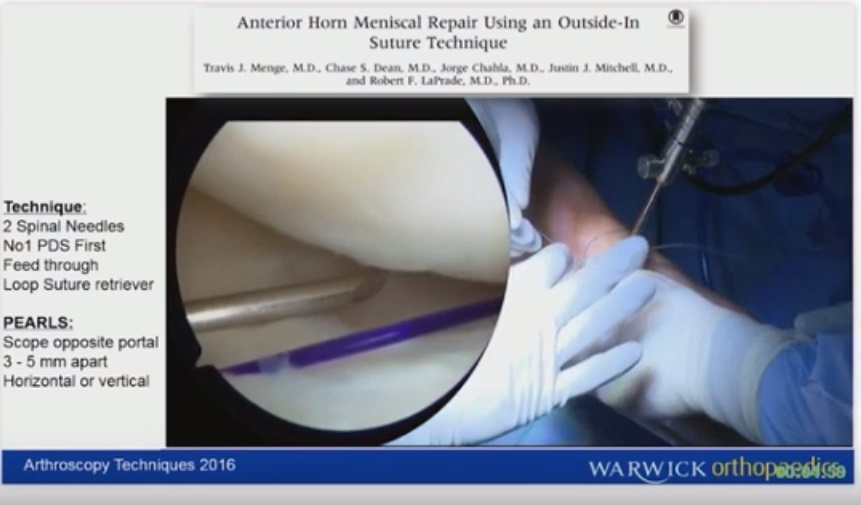
The first stitch is often placed using:
- Inside-out technique
This helps restore meniscal anatomy.
Final Repair
Repair may combine:
- Inside-out sutures
- All-inside devices
Sutures are alternated between:
- Superior surface
- Inferior surface
Technical Pearls
Important Tips
- Ensure stable reduction before final fixation
- Preserve vascular peripheral tissue
- Tie inside-out sutures in full extension
- Use figure-of-four position for lateral compartment access
Biological Augmentation
Common methods discussed include:
- PRP
- Fibrin clot
- Microfracture
Key Insight
Peripheral debridement and creation of a bleeding surface appear more important than biological augmentation alone.
Key Lessons from Chronic Bucket-Handle Tears
- Chronic tears may still be repairable
- Lateral meniscus preservation is critical
- Tissue quality and reducibility determine success
- Meniscectomy should be avoided whenever possible
Discoid Lateral Meniscus Tears
Typical Presentation
- Adolescent athletes
- Locked knee
- Thick discoid meniscus
- Peripheral tears
- Horizontal cleavage tears
Surgical Principles
Saucerization
- Central abnormal portion removed
- Peripheral rim preserved
Recommended rim:
- Approximately 6–8 mm
Repair Strategy
Both components should be repaired:
- Peripheral detachment
- Horizontal cleavage tear
Repairing horizontal tears helps prevent:
- Fluid leakage
- Meniscal cyst formation
Technical Tips
- Use meniscus scorpion device
- Push knots toward periphery
- Visualize needle at all times
- Avoid over-resection
Surgical Sequence
- Saucerization
- Horizontal repair
- Peripheral repair
Ramp Lesions
Definition
Ramp lesions are tears involving:
- Meniscocapsular junction
- Meniscotibial attachment
- Or both
These lesions commonly occur with ACL injuries.
Clinical Importance
Ramp lesions act as secondary stabilizer failures.
If untreated, they may cause:
- Persistent instability
- ACL graft stretching
- ACL graft failure
Diagnosis
Ramp lesions must be actively searched for during arthroscopy.
Diagnostic Techniques
- Modified Gillquist maneuver
- Scope passage between ACL and PCL
- Posteromedial probing
- Use of 70° arthroscope
Important Sign
Visibility of tibial cartilage beneath the posterior horn suggests ramp pathology.
Classification of Ramp Lesions
Small Stable Lesions
- Less than 15 mm
- Acute ACL injuries
These may heal without repair.
Large or Displaced Lesions
- Greater than 15 mm
- Unstable lesions
These generally require repair.
Ramp Repair Techniques
Meniscocapsular Tears
Typically repaired using:
- Anterior all-inside repair
Meniscotibial Tears
Often require:
- Posteromedial portal
- “Shoulder-in-the-knee” technique
Complex Ramp Lesions
Complex lesions may involve:
- Meniscocapsular component
- Meniscotibial component
Management often combines:
- Posterior repair
- Intra-articular all-inside repair
Surgical Pearls for Ramp Repair
- Freshen tissue with rasp and shaver
- Use differential tightening of sutures
- Restore anatomy before final fixation
- Typically requires 3–4 all-inside sutures
Meniscal Root Tears
Importance of Root Tears
Root tears cause loss of meniscal hoop stress function and behave biomechanically similar to total meniscectomy.
Consequences include:
- Meniscal extrusion
- Increased joint contact pressure
- Early arthritis
Types
Medial Root Tears
- Usually degenerative
- Common in middle-aged patients
Lateral Root Tears
- Usually traumatic
- Frequently associated with ACL injury
Root Repair Techniques
Hybrid Repair
Technique includes:
- Cinch suture through transtibial tunnel
- Side-to-side all-inside repair
Advantages:
- Reduces extrusion
- Restores meniscal position
- Minimizes suture cut-through
Suture Tape vs Standard Suture
Advantages of Suture Tape
- Broader surface area
- Less cut-through
- Better footprint compression
Preferred Stitch
- Cinch stitch configuration
Degenerative Root Tears
Surgical Candidates
Repair may be considered if:
- Age < 60 years
- Kellgren-Lawrence grade ? 2
- Acceptable alignment
Avoid Surgery When
- Advanced arthritis
- Severe degeneration
- Elderly low-demand patients
Non-operative management may include:
- Physiotherapy
- Offloader brace
- Injections
Horizontal Cleavage Tears with Meniscal Cyst
Clinical Features
Typical symptoms:
- Pain
- Mechanical catching
MRI may show:
- Horizontal cleavage tear
- Parameniscal cyst
Treatment Strategy
Surgical Steps
- Remove unstable flap
- Debride tear
- Decompress cyst
- Perform trephination
- Approximate superior and inferior leaflets
Important Tip
Avoid overtightening to prevent meniscal crumpling.
Meniscus Repair in Multiligament Injuries
Staged Approach
Stage 1
- Meniscus reduction
- Minimal repair
- MCL repair
Stage 2
- ACL/PCL reconstruction
Biological Advantage
Multiligament injuries produce:
- Large hematoma
- Rich healing environment
This may improve meniscal healing potential.
Meniscus Transplantation
Indications
Primary candidates include young patients with:
- Subtotal meniscectomy
- Total meniscectomy
- Persistent compartment pain
Common Side
Meniscus transplantation is performed more commonly on:
- Lateral side
General Surgical Pearls
Visualization
Lateral Compartment
- Figure-of-four position improves access
Tight Medial Compartments
Consider:
- Alternate portals
- Smaller instruments
- MCL pie-crusting
MCL Pie-Crusting Technique
Indication
- Tight medial compartment during arthroscopy
Technique
- Use 18G needle
- Release area between:
- MCL
- Posterior oblique ligament
Important Warning
Avoid excessively anterior release to prevent postoperative laxity.
Safety Principles During Meniscus Repair
- Keep posterior horn repair at least 10 mm from edge
- Maintain knee at 90° during posterior repair
- Be aware of popliteal artery proximity
- Visualize needles throughout repair
Final Take-Home Messages
- Meniscus preservation should always be prioritized
- Even chronic tears may be repairable
- Tissue quality and reducibility guide treatment decisions
- Proper surgical technique is more important than biological augmentation alone
- Ramp lesions must always be evaluated in ACL-deficient knees
- Root tears should be repaired whenever feasible
- Thorough arthroscopic assessment improves long-term joint preservation
Related Posts
 Tips and Tricks in Meniscal balancing
Tips and Tricks in Meniscal balancingCourtesy: Dr Leonard Ponraj, Dr David Rajan, Arthroscopy Course
- Meniscus Repair : Tips & tricks
Courtesy: Dinshaw Pardiwala, Ashok Shyam, IORG, OrthoTV
 Meniscal Repair using RadioFrequency
Meniscal Repair using RadioFrequencyCourtesy: Rafael Inigo Pavlovich MD, Dr. Pavlovich is the recipient of national honors from several…
Leave a Reply