Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Lumbar Disc Herniation – High-Yield Review
Introduction
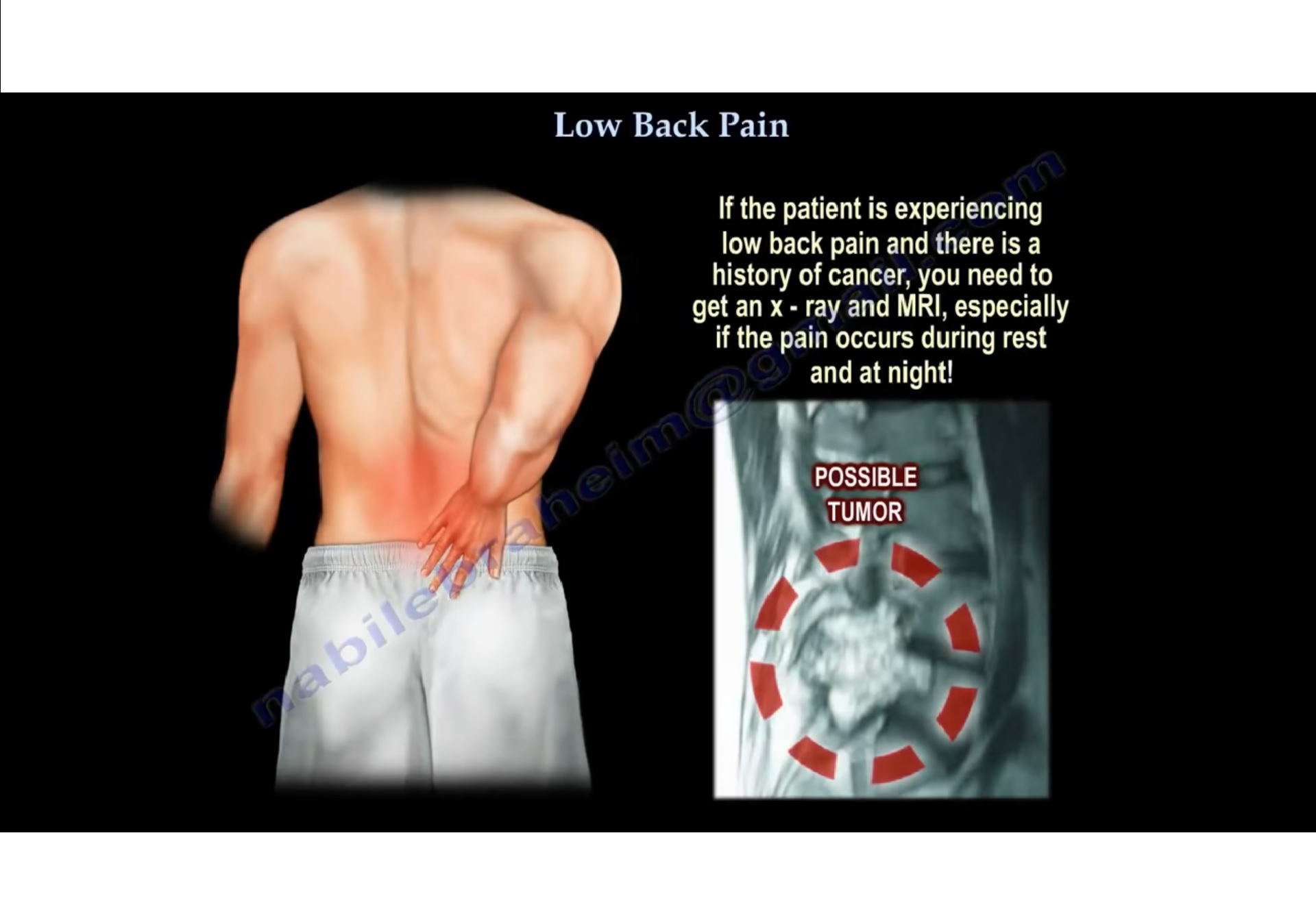
Lumbar disc herniation is one of the most common causes of:
- Low back pain
- Radiculopathy
- Sciatica
Most herniations occur in the lower lumbar spine and may compress adjacent nerve roots, leading to neurological symptoms.
Basic Anatomy
Components of the Spine
The spine consists of:
- Vertebrae
- Intervertebral discs
- Spinal canal
- Neural elements
Neural Anatomy
Spinal Cord
The spinal cord typically ends at:
- T12–L1 level
Conus Medullaris
The terminal portion of the spinal cord is called the:
- Conus medullaris
Cauda Equina
Below the conus lies the:
- Cauda equina
which consists of lumbar and sacral nerve roots.
Lumbar Spine Overview
The lumbar spine contains:
- Five vertebrae: L1–L5
Inferiorly, the lumbar spine articulates with:
- Sacrum
The lumbosacral junction is:
- L5–S1
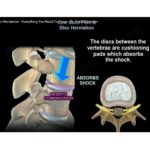
Structure of the Intervertebral Disc
The disc has two major components.
1. Nucleus Pulposus
Characteristics:
- Soft
- Gelatinous
- Shock-absorbing center
2. Annulus Fibrosus
Characteristics:
- Tough fibrous outer ring
- Contains the nucleus pulposus
- Provides structural stability
Common Levels of Herniation
The most commonly affected levels are:
- L5–S1
- L4–L5
These segments experience the greatest mechanical stress.
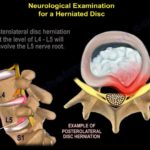
Nerve Root Involvement
Important Rule
- Posterolateral herniation affects the traversing nerve root
- Foraminal herniation affects the exiting nerve root
Common Patterns
| Disc Level | Herniation Type | Affected Nerve Root |
|---|---|---|
| L4–L5 | Posterolateral | L5 |
| L5–S1 | Posterolateral | S1 |
| L4–L5 | Foraminal | L4 |
Types of Disc Herniation
1. Disc Bulge / Protrusion
Characteristics:
- Mild herniation
- Annulus remains intact
2. Disc Extrusion
Characteristics:
- Annulus disrupted
- Disc material extends outward
3. Disc Sequestration
Characteristics:
- Free disc fragment
- No continuity with parent disc
- May undergo spontaneous resorption
Locations of Disc Herniation
Posterolateral Herniation
Most Common Type
Characteristics:
- Compresses a single nerve root
- Produces classic radiculopathy
Foraminal Herniation
Less Common
Occurs in approximately 8–10% of cases.
Characteristics:
- Compresses exiting nerve root
- Often causes severe radicular pain
Central Disc Herniation
Rare but Dangerous
Can compress multiple nerve roots within the cauda equina.
Clinical Features
May cause:
- Severe low back pain
- Bilateral lower limb symptoms
- Bladder dysfunction
- Bowel dysfunction
Central herniation is a neurological emergency.
Cauda Equina Syndrome
Clinical Importance
Cauda equina syndrome is a surgical emergency.
Early recognition is critical because delayed treatment may result in permanent neurological deficit.
Clinical Features
Typical symptoms include:
- Bladder dysfunction
- Bowel dysfunction
- Saddle anesthesia
- Bilateral lower limb weakness
- Bilateral sensory loss
Examination
Important components include:
- Perianal sensation
- Digital rectal examination
- Anal sphincter tone
Investigation
Requires:
- Emergency MRI
Treatment
Management includes:
- Emergency decompression surgery
Timing of surgery strongly influences neurological recovery.
Discogenic Back Pain (Internal Disc Disruption)
Pathophysiology
Occurs due to:
- Annular tear
- Early disc degeneration
without major nerve root compression.
Clinical Features
Typical findings include:
- Pain worsened by sitting
- Pain worsened by flexion
- Limited forward bending
- Relief with extension
Important Difference
Discogenic pain usually does not produce:
- Radiculopathy
- Neurological deficit
Clinical Correlation and MRI
Important Principle
MRI findings must always be correlated with:
- Clinical symptoms
- Physical examination
Imaging abnormalities alone should not determine treatment.
Natural History
Important observations include:
- Many lumbar disc herniations improve spontaneously
- Large extruded discs may resorb over time
- Not all herniations require surgery
Conservative treatment is successful in most patients.
Red Flags in Lumbar Disc Disease
Important warning signs include:
- Cauda equina syndrome
- Progressive neurological deficit
- Severe motor weakness
- Bladder or bowel dysfunction
These findings require urgent evaluation.
Key Clinical Pearls
- Most lumbar disc herniations occur at L4–L5 and L5–S1.
- Posterolateral herniation is the most common pattern.
- Foraminal herniation affects the exiting nerve root.
- Central herniation may cause cauda equina syndrome.
- Discogenic pain differs from radiculopathy.
- MRI abnormalities must always correlate clinically.
- Many disc herniations improve without surgery.
- Early diagnosis of cauda equina syndrome is critical.
Related Posts
 Low Back Ache and Disc Herniation
Low Back Ache and Disc HerniationCourtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
 Low Back Pain. Lumbar Disc Herniation, Causes ,Diagnosis ,Symptoms and Treatment
Low Back Pain. Lumbar Disc Herniation, Causes ,Diagnosis ,Symptoms and TreatmentCourtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
 Low back ache and Disc herniation
Low back ache and Disc herniationCourtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Leave a Reply