Courtesy: Marco Guidi MD, University Hospitals Zurich, Switzerland
Introduction
Intramedullary fixation is an emerging minimally invasive technique for managing fractures of the metacarpals and phalanges.
It serves as an alternative to plate fixation, though treatment choice must always be guided by:
- Fracture pattern
- Stability requirements
- Soft-tissue considerations
Limitations of Plate Fixation
Common Complications
- Finger stiffness
- Extensor tendon adhesion
- Impaired tendon gliding
Mechanism
- Dorsal plates may interfere with:
- Extensor tendon movement
- Soft tissue gliding
Leads to:
- Extensor lag
- Postoperative stiffness
Evidence
- Earlier studies reported significant stiffness, especially in proximal phalanx fractures
- Modern low-profile plates reduce but do not eliminate this issue
Emergence of Intramedullary Fixation
Concept
Intramedullary fixation aims to:
- Minimize soft tissue dissection
- Preserve tendon gliding
- Enable early mobilization
Historical Development
- Early reports demonstrated success in metacarpal fractures
- Later popularized with minimally invasive techniques and improved outcomes
Current Evidence
- Increasing literature:
- ~85 studies (metacarpals)
- ~36 studies (phalanges)
- Studies show good functional outcomes
Indications
Suitable Fracture Types
- Transverse fractures
- Short oblique fractures
- Selected comminuted fractures
- Fractures where soft-tissue preservation is important
Not Suitable For
- Long oblique fractures
- Spiral fractures
- Very proximal or distal fractures
Reason: Limited bone stock for screw purchase
Implants Used
Common Implants
- Headless compression screws (HCS)
- Self-drilling, self-tapping screws
Typical Sizes
- 3.0 mm — Metacarpals
- 2.2 mm — Phalanges
- 1.7 mm — Small phalanges
Surgical Technique
General Principles
- Closed or minimally invasive reduction
- Small incision
- Guidewire insertion into medullary canal
- Cannulated screw insertion over guidewire
Metacarpal Fracture Fixation
Entry Point
- Through dorsal metacarpal head
Technique Steps
- Achieve reduction
- Insert guidewire
- Advance into canal
- Insert screw across fracture
Key Considerations
- Accurate length measurement
- Confirm position on AP and lateral fluoroscopy
- Screw should cross the isthmus for stability
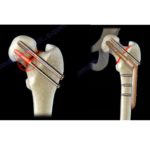
Comminuted Fractures
Y-Strut Concept (Del Piñal)
- Uses two screws to create a triangular construct
Advantages
- Improved stability
- Better resistance to deforming forces
Phalangeal Fractures
Proximal Phalanx
Techniques
1. Transarticular Antegrade
- Entry via metacarpal head
Drawback: Risk of cartilage injury
2. Retrograde Intra-articular
- Entry through phalanx head
Advantages
- Simple
- Quick
Risks
- Cartilage injury
- Central slip injury
Middle Phalanx
Antegrade Extra-articular
- Entry from lateral side
- Avoids cartilage injury
Retrograde Intra-articular
- Entry via DIP joint
Risk of extensor tendon injury
Postoperative Management
Early Mobilization
- Encouraged with protected movement
Additional Support
- Buddy taping for ~6 weeks
Rehabilitation
- Early hand therapy improves outcomes
Follow-Up
- X-ray at 6 weeks
- Manual work: ~8 weeks
- Office work: 1–2 weeks
Outcomes
Systematic Review Findings
- 958 fractures analyzed
- Operative time: ~26 minutes
- Healing time: 5–6 weeks
- Complication rate: ~3.2%
Most Common Complication
- Extension lag (~2%)
Overall Results
- Good range of motion
- Faster recovery
Cartilage Injury
Findings
- 4–9% cartilage damage reported
Clinical Significance
- Long-term osteoarthritis risk remains unclear
- Requires further research
Tendon Injury
Risk Factors
- Blind percutaneous insertion
Prevention
- Mini-open approach (<1 cm incision)
- Reduces tendon injury risk
Complications
- Screw protrusion
- Screw breakage
- Rotational instability
- Loss of length
- Extension lag
- Rare osteonecrosis
Contraindications
- Long oblique fractures
- Spiral fractures
- Highly comminuted intra-articular fractures
- Open physes
- Active infection
- Subacute fractures
Advantages of Intramedullary Fixation
- Minimally invasive
- Short operative time
- Less soft tissue disruption
- Reduced edema
- Faster rehabilitation
- Stable fixation for early motion
Limitations
- Not suitable for all fracture types
- Risk of cartilage injury
- Difficult removal of broken screws
Key Take-Home Messages
- Intramedullary fixation is a safe and effective technique for selected fractures
- Provides minimally invasive stabilization with early mobilization
- Proper fracture selection is critical
- Plate fixation remains necessary for complex fracture patterns


Thanks