Courtesy: Marco Guidi MD, University Hospitals Zurich, Switzerland
Introduction
- Intramedullary fixation is an emerging technique for the treatment of metacarpal and phalangeal fractures.
- It is considered a minimally invasive alternative to traditional plate fixation.
- However, plate fixation is still relevant, and treatment should always be based on proper fracture indication and pattern.
Limitations of Plate Fixation
Major complications
- Finger stiffness
- Extensor tendon adhesion and scarring
- Reduced tendon gliding over the plate
Mechanism
- Plates placed dorsally may interfere with:
- Extensor tendon movement
- Soft-tissue gliding
- This may result in:
- Extensor lag
- Postoperative stiffness
Evidence
- Earlier studies (e.g., Page & Stern, 1998) reported significant stiffness after plate fixation, particularly in proximal phalanx fractures.
- Although modern low-profile plates have reduced these complications, stiffness still remains a concern in some cases.
Emergence of Intramedullary Fixation
- Intramedullary screw fixation aims to:
- Reduce soft-tissue dissection
- Preserve tendon gliding
- Allow earlier rehabilitation.
Early reports
- Bolton et al. (2010) reported successful treatment of subcapital metacarpal fractures using intramedullary screws.
Further development
- Francisco del Piñal popularized minimally invasive intramedullary fixation with excellent clinical outcomes.
Current Literature
- Over the past decade there has been a significant increase in publications regarding intramedullary fixation.
- Approximate literature trends:
- ~85 studies on metacarpal intramedullary fixation
- ~36 studies on phalangeal fractures.
- Biomechanical and clinical studies from several centers, including Zurich, have reported good functional outcomes.
Indications
Intramedullary screw fixation is most suitable for:
- Transverse fractures
- Short oblique fractures
- Selected comminuted fractures
- Fractures where minimal soft-tissue dissection is preferred
Not ideal for
- Long oblique fractures
- Spiral fractures
- Very proximal fractures
- Very distal fractures
Reason:
- Limited bone stock for adequate screw purchase.
Implants Used
Commonly used implants include:
- Headless compression screws (HCS)
- Self-drilling and self-tapping screws
Typical sizes:
- 3.0 mm screws – metacarpals
- 2.2 mm screws – phalanges
- 1.7 mm screws – small phalanges
Surgical Technique
General principles
- Perform closed or minimally invasive fracture reduction.
- A small incision is made over the joint.
- A guide K-wire is inserted into the intramedullary canal.
- A cannulated headless compression screw is advanced over the wire to stabilize the fracture.
Metacarpal Fracture Fixation
Entry point
- Through the dorsal aspect of the metacarpal head.
Technique steps
- Achieve fracture reduction.
- Insert guidewire through the metacarpal head.
- Advance into the intramedullary canal.
- Insert cannulated screw across the fracture.
Key technical considerations
- Measure metacarpal length carefully.
- Confirm position in AP and lateral fluoroscopic views.
- Ideally, the screw should cross the isthmus of the canal for stability.
Comminuted Fractures
- Some comminuted fractures may still be treated with intramedullary fixation.
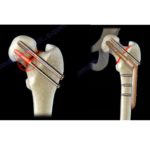
Y-Strut Concept (Del Piñal)
- Uses two intramedullary screws to create a triangular or Y-shaped structural stability.
- Provides:
- Improved stability
- Better resistance to deforming forces.
Proximal Phalanx Fractures
Screw size
- Usually 2.2 mm screws
Technique options
- Transarticular Antegrade Technique
- Guidewire inserted through metacarpal head ? proximal phalanx.
- Screw passed across fracture.
Drawback
- Potential cartilage injury at entry point.
- Retrograde Intra-articular Technique
- Finger flexed at PIP joint.
- Screw inserted through phalanx head proximally.
Advantages:
- Simple
- Fast
- Frequently used technique.
Potential risks:
- Cartilage injury
- Central slip injury
Middle Phalanx Fractures
Antegrade extra-articular technique
- Entry from lateral side.
- Avoids cartilage injury.
- Suitable for transverse fractures.
Retrograde intra-articular technique
- Entry through distal interphalangeal joint.
Risks:
- Extensor tendon injury
Postoperative Management
Early mobilization
- Early protected motion encouraged.
Additional protection
- Buddy taping for 6 weeks to control rotational instability.
Rehabilitation
- Early hand therapy improves outcomes.
Follow-up protocol
- X-ray at 6 weeks
- Return to manual activity at ~8 weeks
- Office work possible within 1–2 weeks.
Outcomes
Systematic review findings:
- 958 fractures analyzed
- Mean operative time: ~26 minutes
- Fracture healing: 5–6 weeks
- Complication rate: ~3.2%
Most common complication
- Extension lag (~2%)
Overall results show:
- Good range of motion
- Rapid recovery.
Cartilage Damage
Studies report limited cartilage injury at entry point:
- 4–5% surface damage with larger screws.
- Other studies report 4–9% cartilage loss.
Clinical significance
- Long-term risk of post-traumatic osteoarthritis remains unclear.
- Long-term outcome studies are still limited.
Tendon Injury
Risk factors:
- Percutaneous insertion without visualization.
Evidence suggests:
- Mini-open approach (<1 cm incision) reduces extensor tendon injury compared with purely percutaneous technique.
Complications
Possible complications include:
- Screw protrusion
- Screw breakage
- Rotational instability
- Loss of fracture length
- Extension lag
- Rare osteonecrosis of phalanx head
Contraindications
Intramedullary fixation should not be used for:
- Long oblique fractures
- Spiral fractures
- Highly comminuted intra-articular fractures
- Open growth plates
- Active infection
- Subacute fractures.
Advantages of Intramedullary Fixation
- Minimally invasive
- Short operative time
- Less soft-tissue disruption
- Lower postoperative edema
- Faster rehabilitation
- Adequate stability for early motion.
Limitations
- Not suitable for all fracture patterns.
- Potential cartilage injury during screw entry.
- Removal of broken screws can be technically challenging.
Key Take-Home Messages
- Intramedullary screw fixation is a safe and effective technique for selected metacarpal and phalangeal fractures.
- It offers minimally invasive stabilization with early rehabilitation.
- Appropriate patient and fracture selection is essential for optimal outcomes.
- Plate fixation still remains necessary for complex fracture patterns.


Thanks