Courtesy: Prof Joseph Queally, MD, FRCS Tr and Orth, M Ed
Dublin, Ireland
PELVIC FRACTURES – MANAGEMENT
AIMS
- PREVENT MORTALITY
– hemorrhage control - PREVENT MORBIDITY
– early recognition/management of soft tissue, urological, neurological injuries
Mortality
- 5% mortality rate in pelvic fractures
Predictors of Mortality:
- Older patient-Age > 60
- SBP < 90mmHg on arrival
- Severely displaced fractures (posterior displacement, APC III)
- 4 unit RCC transfusion
- 50% of severe pelvic fractures have bleeding source than pelvic Fracture
CLOSE –FILL- FIND
- Provide Initial Pelvic Stability using a BINDER (Immediate when pelvic injury Suspected)
- Fill with Blood (Tranexamic Acid, Transfusion)
EXTERNAL FIXATOR
- (rarely required… open book Or post laparotomy/packing)
TRACTION
- very rarely required… Vertical shear injury
C Clamp
(almost never required..
Unstable posterior injury)
BINDER
- LIFE SAVING DEVICE
- Stabilises pelvis via Circumferential Compression and Tamponade effect
- Reduces pelvic volume
- Apply at level of GT NOT ILIAC WING
- Use Binder or simple sheet
- Consider internal rotating lower limbs and tie sheet around Knees
BINDER CARE
- LEAVE IN PLACE UNTIL PATIENT STABLE (haemodynamically)
- TRY TO REMOVE AFTER 6 HOURS, monitor BP/HR, if still unstable replace
- OK TO LEAVE ON IF STILL HEMODYNAMICALLY UNSTABLE BUT MUST CARRY OUT SKIN CARE
- Do not over-compress
- Check (loosen slightly to access pressure areas)
- Every 6 hours pad pressure points
EXTERNAL FIXATION (RARELY REQUIRED, as pelvic binder achieves same function)
Indications :
- Unstable pelvis (some open books.. unstable with binder)
- Post laparotomy/packing
- Open fractures
How to apply :
- Iliac wing or Supracetabular Pins
Iliac Wing
- Easier/quicker
- Less Control
Supra-acetabular(through the SupraAcetabular Corridor: AIIS to Sciatic Buttress)
- Need imaging
- Better control (posterior pelvis) and stability
- technically demanding, with higher rater of complications
- ENSURE POSITION ALLOWS PATIENT TO BE NURSED/SIT
C Clamp
WHEN: NEVER/ALMOST NEVER
- Severe posterior injuries
- Dislocated Sl joint/vertical shear that remains unstable despite binder and Resuscitation
Advantages :
- Good posterior stability
Disadvantages : Not easy
- Need imaging
- Complication risk
Pelvic Haemorrhage
- 80% presacral venous plexus
- 20% arterial (internal iliac SGA, obturator artery, obturator)
EMBOLISATION
- 85- 90 % effective in controlling pelvic fracture related Haemorrhage
- Works well for arterial bleeding, not so well for venous bleeding
- 10% of all pelvic fractures require embolization
- Rapid embolization… Within 3 hours of arrival (36.4% v 75% mortality)
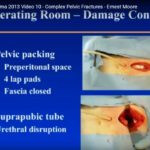
PELVIC PACKING
- Last resort…. Very rarely required
WHEN:
- Patients with arterial bleeding who are unstable despite binder, and embolization
- Unstable venous bleeding not amenable to angiography
- Exsanguinating bleeding/non responders who have damage control laparotomy
HOW:
- Stoppa approach
- Laparotomy
SKIN
- Always check for OPEN FRACTUREs
- MUST INSPECT SKIN AREA CIRCUMFERENTIALLY INCLUDING PERINEUM
Check for Rectal injury (PR bleeding), Vaginal injury (PV bleeding), Scrotal injury - DO NOT MISS OPEN FRACTURE….. mortality up to 50%
Give IV antibiotics, tetanus etc, early debridement
MOREL LAVELLE LESION
- Degloving injury where skin + subcutaneous tissue separates from fascia
- easy to miss as often closed injury
- significant morbidity + infection risk if missed
- bruising + fluctuance
- Smaller lesions can be managed conservatively
- larger need debridement, vac dressing + drain, OrthoPlastic Approach
UROLOGICAL INJURY
Any suspicion of urological injury (blood at meatus, high riding Prostate, haematuria) call urology and arrange imaging
ATTEMPT SINGLE PASS OF CATHETER (16Fr)…
- If successful and suspicious of injury, imaging required :
Retrograde cystogram
CT cystogram (gold standard) - If unsuccessful, perform retrograde urethrogram using catheter tip
With balloon and call urology team to place suprapubic catheter
(out of zone of Stoppa incision) via US technique
Retrograde urethrogram/
- Used if Unable to pass catheter
- Identifies urethral injury
Retrograde Cystogram:
- Used if blood seen in urine
- Identifies bladder injury
Neurological Injury
MUST EXAMINE & DOCUMENT
- L5 nerve root
- Sacral nerve roots
- LFCN ( lateral femoral cutaneous nerve)

Leave a Reply