Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Pelvic Fracture Classification: Young–Burgess and Tile Systems
Introduction
Pelvic fracture classification is essential to determine:
- Severity of injury
- Pelvic stability
- Risk of hemorrhage
- Need for surgical intervention
Clinical Importance
Initial pelvic X-ray and patient condition help classify injuries as:
- Stable (simple)
- Unstable (life-threatening) ? requires urgent resuscitation
Common Classification Systems
1. Young–Burgess Classification
- Based on mechanism of injury
- Reflects direction of force
2. Tile Classification
- Based on pelvic stability
Young–Burgess Classification
Types
- Lateral Compression (LC)
- Anteroposterior Compression (APC)
- Vertical Shear (VS)
Lateral Compression (LC)
Mechanism
- Internal rotation force on pelvis
LC Type I
Features
- Sacral compression fracture
- Pubic ramus fracture
Stability
- Usually stable
LC Type II
Features
- Crescent fracture of iliac wing
- Posterior sacroiliac ligament injury
Stability
- Rotationally unstable
LC Type III (Windswept Pelvis)
Features
- LC injury on one side
- APC injury on opposite side
Mechanism
- High-energy trauma (e.g., rollover accidents)
Clinical Significance
- LC I & II – deaths often due to head injury
- LC III – associated with bowel injury
Anteroposterior Compression (APC)
Mechanism
- External rotation force
- Direct pelvic impact or forced leg abduction
Key Feature
Symphysis pubis diastasis (“open-book pelvis”)
APC Type I
Features
- Symphyseal widening < 2.5 cm
- Ligaments intact
Stability
- Rotationally & vertically stable
Treatment
- Conservative
APC Type II
Features
- Symphyseal widening > 2.5 cm
- Injury to:
- Sacrospinous ligament
- Sacrotuberous ligament
- Anterior SI ligaments
Stability
- Rotationally unstable
- Vertically stable
APC Type III
Features
- Complete disruption including posterior SI ligaments
Stability
- Rotationally + vertically unstable
Clinical Importance
Highest risk of:
- Severe hemorrhage
- Hemorrhagic shock
Vertical Shear (VS)
Mechanism
- Vertical force (e.g., fall from height)
Features
- Disruption of:
- Sacroiliac ligaments
- Pelvic floor
Stability
- Rotationally unstable
- Vertically unstable
Clinical Significance
Associated with:
- Massive bleeding
- High mortality
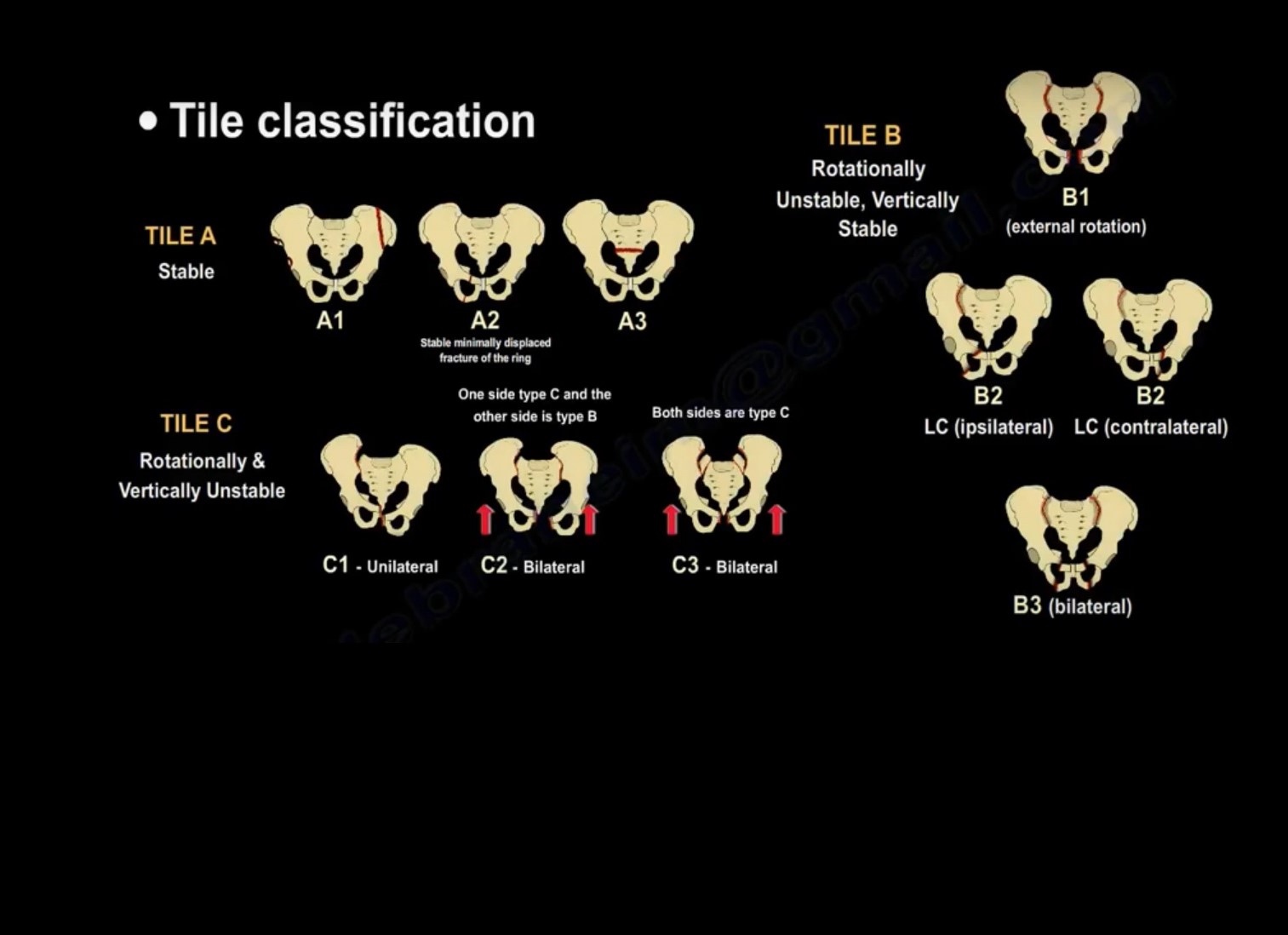
Tile Classification
Concept
Based on pelvic stability
Types
Type A – Stable
Examples
- ASIS avulsion (Sartorius)
- AIIS avulsion (Rectus femoris)
- Iliac wing fracture
- Transverse sacral fracture
Stability
- Pelvic ring intact
Management
- Conservative
Type B – Rotationally Unstable, Vertically Stable
Examples
- Open-book injury
- Lateral compression injury
- Bucket-handle injury
Features
- Rotational instability only
Type C – Rotationally and Vertically Unstable
Features
- Complete disruption of pelvic ring
- Severe instability
Clinical Importance
High risk of:
- Major hemorrhage
- Life-threatening injury
Bleeding in Pelvic Fractures
Major Causes of Mortality
- Hemorrhagic shock
- Associated injuries
Risk Factors
- Age > 60 years
- Open fractures
- High Injury Severity Score (ISS)
Source of Bleeding
Venous (90%)
- Cancellous bone
- Pelvic venous plexus
Arterial (10%)
- Superior gluteal artery
- Obturator artery
- Internal pudendal artery
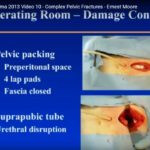
Emergency Management
Pelvic Binder
Indication
- Open-book (APC) injuries
Function
- Reduces pelvic volume
- Controls hemorrhage
Massive Transfusion Protocol
Ratio
- Packed RBC : Plasma : Platelets = 1 : 1 : 1
Angiography and Embolization
Indications
- ~20% of APC and VS injuries
- ~2% of LC injuries
Surgical Stabilization
Indications
- Unstable pelvic fractures
Anterior Fixation
- Multihole plate
Posterior Fixation
- Percutaneous sacroiliac screws
Key Exam Points
Classification Basis
| Classification | Based On |
|---|---|
| Young–Burgess | Mechanism of injury |
| Tile | Pelvic stability |
High-Yield Concepts
- APC III and VS – highest bleeding risk
- LC injuries – often associated with head injury
- 90% bleeding is venous
- Pelvic binder is critical in open-book injuries
Clinical Insight
Always assess:
- Stability
- Hemodynamic status
These guide:
- Resuscitation
- Definitive management
Leave a Reply