Courtesy: Dr Amr Abdelgawad, Paediatric Orthopaedic Surgeon,University of Texas, USA
Intoeing in Children
Overview
- Intoeing is a common pediatric gait pattern where:
- Feet point inward during walking
- Also known as:
- “Pigeon-toed gait”
Clinical Importance
- One of the most common reasons for pediatric orthopaedic consultation
- Most cases are:
- Physiological
- Self-resolving
Objectives of Evaluation
- Understand normal rotational alignment
- Differentiate:
- Physiologic vs pathologic causes
- Identify underlying anatomical source
Main Causes of Intoeing
Three Anatomical Levels
| Location | Cause |
|---|---|
| Femur | Excess femoral anteversion |
| Tibia | Internal tibial torsion |
| Foot | Metatarsus adductus |
Clinical Evaluation of Intoeing
1. Foot Progression Angle (FPA)
Definition
- Angle between:
- Foot axis
- Direction of walking
Interpretation
| Value | Meaning |
|---|---|
| Positive | Out-toeing |
| Negative | Intoeing |
Clinical Tip
- Observe:
- Walking
- Running
- Repeat multiple times (children may alter gait in clinic)
2. Hip Rotation Assessment
Method
- Child prone
- Knees flexed to 90°
Movements
| Foot Movement | Hip Motion |
|---|---|
| Foot outward | Internal rotation |
| Foot inward | External rotation |
Normal
- Internal ? external rotation
Abnormal
- Internal rotation >70°
- External rotation <30°
Suggests femoral anteversion
3. Tibial Rotation (Thigh-Foot Angle)
Method
- Observe angle between:
- Thigh
- Foot
Normal
- 5–10° external rotation
Abnormal
- Internal angle — internal tibial torsion
4. Forefoot–Hindfoot Relationship
Assessment
- Heel bisector line
Normal
- Passes between 2nd and 3rd toes
Severity (Metatarsus Adductus)
| Position | Severity |
|---|---|
| 3rd toe | Mild |
| 4th toe | Moderate |
| 5th toe | Severe |
Additional Finding
- Curved lateral border of foot
Causes in Detail
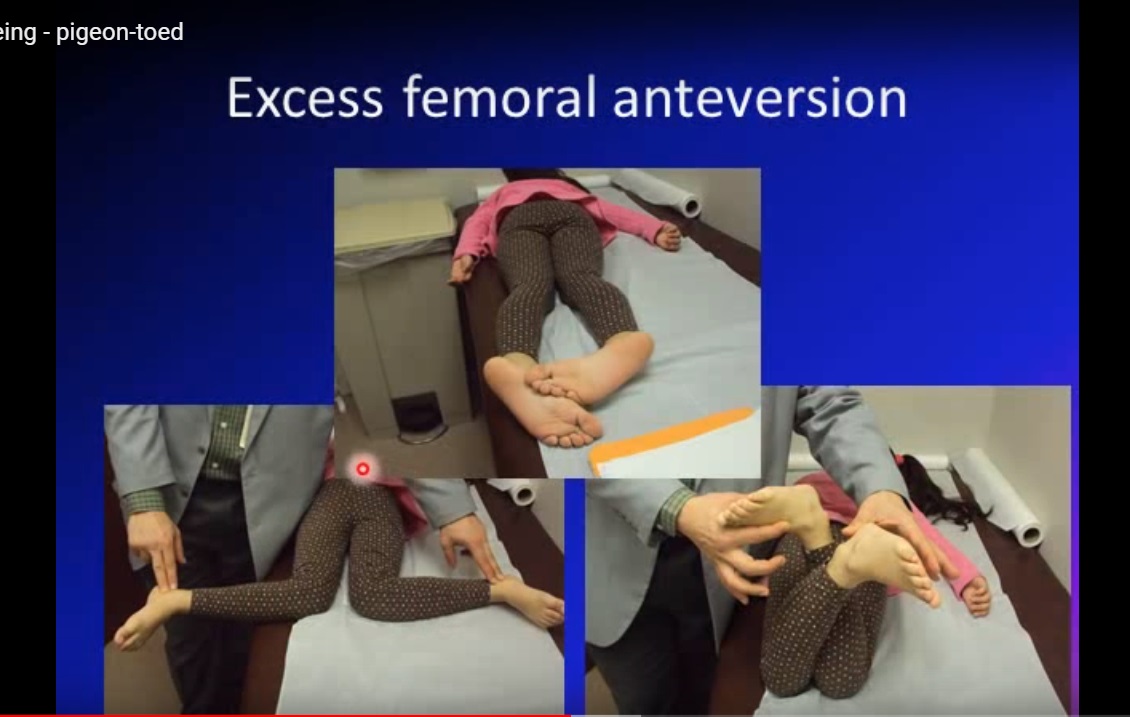
1. Excess Femoral Anteversion
Definition
- Increased angle between femoral neck and shaft
Normal Development
| Age | Anteversion |
|---|---|
| Birth | ~40° |
| Adult | ~15–17° |
Epidemiology
- Most common cause in 3–8 years
Clinical Features
- Increased internal rotation
- Decreased external rotation
- “W-sitting” posture
Treatment
- Observation only
Natural History
- Resolves by ~8 years
Surgery
- Rare:
- Femoral derotation osteotomy
2. Internal Tibial Torsion
Definition
- Internal rotation of tibia
Epidemiology
- Most common cause in <3 years
Cause
- Intrauterine positioning
Clinical Findings
- Normal hip rotation
- Abnormal thigh-foot angle
Treatment
- Observation
Natural History
- Resolves by ~4 years
3. Metatarsus Adductus
Definition
- Medial deviation of forefoot
Clinical Features
- Curved lateral foot border
- Normal hindfoot
Differentiation from Clubfoot
| Feature | Metatarsus Adductus | Clubfoot |
|---|---|---|
| Forefoot | Adducted | Adducted |
| Hindfoot | Normal | Varus |
| Ankle | Normal | Equinus |
Associated Conditions
- Developmental dysplasia of the hip (DDH)
- Always assess hips
Treatment of Metatarsus Adductus
Flexible Deformity
- Observation
Persistent (>6 months)
- Orthopaedic referral
- Casting or bracing
Adjunct
- Straight-last shoes
Surgery
- Rare
Summary Table
| Cause | Age Group | Treatment |
|---|---|---|
| Femoral anteversion | 3–8 years | Observation |
| Internal tibial torsion | <3 years | Observation |
| Metatarsus adductus | Infants | Observation ± casting |
Key Clinical Point
- Most intoeing cases are normal developmental variations
- Require:
- Reassurance
- Observation

Leave a Reply