Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Gluteus Medius Tendon Tears
Introduction
Gluteus medius tendon tears are an increasingly recognized cause of lateral hip pain and disability. Historically, many of these patients were diagnosed with trochanteric bursitis, but advances in imaging and understanding of hip biomechanics have shown that gluteus medius pathology is a common underlying cause.
Gluteus medius tears form an important part of Greater Trochanteric Pain Syndrome (GTPS) and should be considered in any patient with persistent lateral hip pain.
Greater Trochanteric Pain Syndrome (GTPS)
GTPS represents a spectrum of disorders affecting the peritrochanteric region.
This continuum includes:
- Trochanteric bursitis
- Gluteus medius tendinitis
- Gluteal tendinosis
- Partial-thickness tendon tears
- Full-thickness tendon tears
- Chronic retracted tears with muscle atrophy
Recognition of this spectrum is important because treatment and prognosis vary depending on the stage of disease.
Etiology and Risk Factors
Gluteus medius tendon tears are most commonly seen in older adults and are frequently associated with degenerative changes around the hip.
Common Risk Factors
- Advanced age
- Hip osteoarthritis
- Degenerative tendon disease
- Chronic overuse
- Altered hip biomechanics
Many patients remain asymptomatic during the early stages of disease, allowing gradual progression before diagnosis.
Clinical Presentation
Symptoms
Patients typically present with:
- Chronic lateral hip pain
- Insidious onset of symptoms
- Pain radiating to the buttock
- Pain radiating to the lower back
- Difficulty with prolonged walking or standing
Physical Examination Findings
Common examination findings include:
- Tenderness over the greater trochanter
- Limping gait
- Weakness of hip abduction
- Positive Trendelenburg sign
- Trendelenburg gait in advanced cases
Why Diagnosis Is Often Missed
Diagnosis may be delayed for months or even years because:
- Symptoms are often vague and nonspecific
- Hip abductor strength may remain normal or only mildly reduced
- Findings may mimic trochanteric bursitis
- Patients frequently undergo repeated treatment without addressing the underlying tendon pathology
Persistent “trochanteric bursitis” that fails to improve should raise suspicion for a gluteus medius tendon tear.
Differential Diagnosis
Several conditions can produce symptoms similar to gluteus medius pathology and should be excluded.
Important Differential Diagnoses
- Stress fractures
- Avascular necrosis of the femoral head
- Hip osteoarthritis
- Femoroacetabular impingement (FAI)
- Lumbar spine pathology
- Lumbar radiculopathy
A comprehensive clinical assessment is essential before confirming the diagnosis.
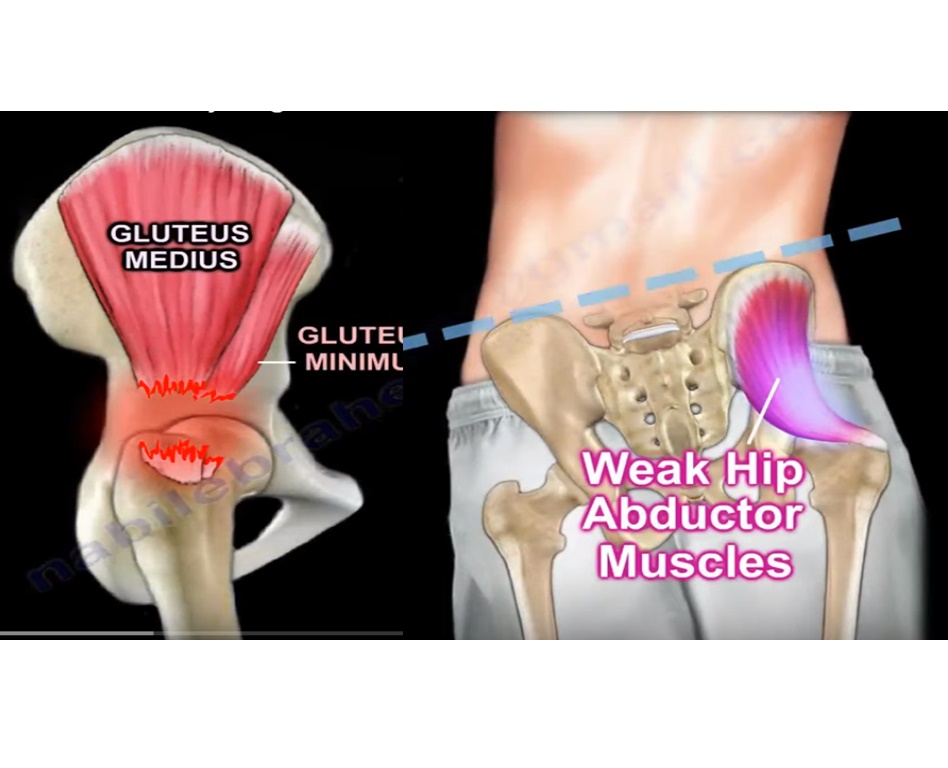
Hip Abductor Biomechanics
Primary Hip Abductors
The hip abductor mechanism consists primarily of:
- Gluteus medius
- Gluteus minimus
These muscles play a critical role in pelvic stability during the stance phase of gait.
Consequences of Abductor Weakness
When the abductors become dysfunctional:
Trendelenburg Sign
The pelvis drops on the contralateral side during single-leg stance.
Abductor Lurch
To compensate for weakness, patients lean their trunk toward the affected side.
This compensatory mechanism:
- Reduces the abductor moment arm
- Decreases muscular demand
- Helps maintain balance during walking
Diagnosis
Clinical Suspicion
The diagnosis should be suspected in patients with:
- Chronic lateral hip pain
- Persistent symptoms despite treatment
- Recurrent or refractory trochanteric bursitis
Imaging
MRI: Investigation of Choice
MRI is the most useful imaging modality for evaluating gluteus medius pathology.
MRI can identify:
- Tendinosis
- Partial-thickness tears
- Full-thickness tears
- Tendon retraction
- Fatty degeneration
- Muscle atrophy
MRI remains valuable even in patients who have undergone previous hip arthroplasty.
Surgical Anatomy
Understanding tendon insertion anatomy is essential when planning repair.
Greater Trochanter Facets
Anterior Facet
Insertion of the gluteus minimus tendon.
Lateral Facet
Insertion of the gluteus medius tendon.
Superoposterior Facet
Additional insertion of the gluteus medius tendon.
Posterior Facet
Insertion area for the gluteus maximus.
Knowledge of these insertion sites guides anchor placement and surgical repair techniques.
Natural History
Gluteus medius tendon disease is generally progressive.
Typical progression includes:
- Tendinosis
- Partial-thickness tear
- Full-thickness tear
- Tendon retraction
- Fatty infiltration
- Muscle atrophy
Early diagnosis and intervention are associated with better outcomes because chronic tears become increasingly difficult to repair.
Treatment
Conservative Management
Conservative treatment remains the first-line approach for most patients without significant tendon tearing.
Treatment Options
- Physiotherapy
- Activity modification
- Nonsteroidal anti-inflammatory drugs (NSAIDs)
- Hip abductor strengthening programs
Many patients with tendinosis or mild disease improve with non-operative treatment.
Indications for Surgery
Surgical intervention may be considered when patients have:
- Symptomatic tendon tears
- Functional disability
- Persistent pain despite adequate conservative treatment
- Progressive weakness
Surgical Treatment Options
Primary Tendon Repair
Indications
- Partial-thickness tears
- Repairable full-thickness tears
Outcomes
Primary repair generally provides:
- Significant pain relief
- Improved hip function
- Better gait mechanics
- Restoration of abductor strength
Early repairs tend to produce the best results.
Irreparable Tears
Certain tears may not be suitable for direct repair.
Features of Irreparable Tears
- Severe tendon retraction
- Advanced fatty degeneration
- Significant muscle atrophy
- Chronic longstanding tears
Reconstruction and Tendon Transfer Procedures
When direct repair is not possible, reconstruction techniques may be considered.
Gluteus Maximus Transfer
The most commonly performed reconstruction procedure.
Advantages
- Similar muscle fiber orientation
- Effective restoration of abductor function
- Reliable pain relief
Other Reconstruction Options
Vastus Lateralis Transfer
May be used in selected cases.
Achilles Tendon Allograft Reconstruction
Reserved for complex situations requiring tissue augmentation.
Special Clinical Situations
Persistent Limp After Total Hip Replacement
Patients who continue to limp after hip arthroplasty should be evaluated for:
- Gluteus medius tendon tear
- Abductor insufficiency
MRI can be particularly helpful in these cases.
Superior Gluteal Nerve Injury
Abductor dysfunction caused by superior gluteal nerve injury has a poorer prognosis and may not respond well to tendon repair alone.
Prognostic Factors
Factors Associated With Better Outcomes
- Early diagnosis
- Minimal muscle atrophy
- Limited fatty degeneration
- Repairable tendon tissue
- Early surgical intervention when indicated
Factors Associated With Poor Outcomes
- Chronic tears
- Severe tendon retraction
- Significant fatty infiltration
- Advanced muscle atrophy
- Superior gluteal nerve dysfunction
Key Takeaways
- Gluteus medius tendon tears are a common but frequently overlooked cause of lateral hip pain.
- Many cases previously diagnosed as trochanteric bursitis are actually part of the GTPS spectrum.
- MRI is the investigation of choice and accurately identifies tendon pathology and muscle quality.
- Hip abductor weakness can result in Trendelenburg gait and significant functional limitations.
- Early diagnosis and treatment improve outcomes and may prevent progression to irreparable tears.
- Primary repair offers excellent results for most repairable tears.
- Chronic retracted tears with severe atrophy may require tendon transfer or reconstructive procedures.
Leave a Reply