Courtesy: Kaye Wilkins MD, Prof Lynn Staheli MD, www.global-help.org
Pediatric Hip Fractures (Proximal Femur Fractures)
Overview
- Rare injuries in children, accounting for less than 1% of pediatric fractures
- Usually caused by high-energy trauma
- Associated with significant complications, especially avascular necrosis (AVN)
Pediatric vs Adult Femoral Neck Fractures
| Feature | Pediatric | Adult |
|---|---|---|
| Incidence | Rare | Common |
| Mechanism | High-energy trauma | Often low-energy |
| Blood supply | Vulnerable | More stable |
| Complications | High AVN risk | Lower AVN risk |
| Treatment priority | Urgent fixation | Early mobilization |
Delbet Classification
Delbet classification
| Type | Description |
|---|---|
| I | Transphyseal |
| II | Transcervical |
| III | Cervicotrochanteric |
| IV | Intertrochanteric |
Additional clinically important groups include:
- Neonatal fractures
- Pathological fractures
- Stress fractures
Anatomy and Growth Considerations
Ossification Centers
- Initially, the femoral head and greater trochanter share a common ossification center
- Later they separate into distinct centers
- Persistent connecting cartilage contributes to unique pediatric fracture patterns
Blood Supply – Most Important Concept
Infant (<4–6 months)
- Blood vessels freely cross the physis
- Blood supply is relatively preserved
After Approximately 3 Years
- Physis becomes a vascular barrier
- Blood supply mainly depends on:
- Medial circumflex femoral artery
- Posterior-superior retinacular vessels
Clinical Importance
- These vessels run along the femoral neck
- Easily injured during fracture
- Major reason for AVN risk
Mechanism of Injury
Most commonly due to:
- Road traffic accidents
- Fall from height
- Child abuse, especially in infants
Delbet Fracture Types in Detail
Type I – Transphyseal Fracture
Most Severe Injury
- Highest risk of AVN
- May occur:
- With dislocation
- Without dislocation
Clinical Features
Can mimic:
- Developmental dysplasia of the hip
Important differentiating features:
- Pain
- Swelling
- Movement at the physis during examination
Treatment
- Gentle reduction
- Pavlik harness in infants
- Avoid aggressive fixation
Complications
- AVN
- Coxa vara
- Retroversion deformity
Type II – Transcervical Fracture
Most Common Type
Treatment
- Orthopedic emergency
- Closed or open reduction
- Cannulated screw fixation
AVN Risk
- Approximately 15–40%
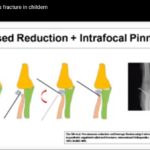
Type III – Cervicotrochanteric Fracture
Features
- More stable than Type II
- Muscle forces produce:
- Flexion deformity from iliopsoas
- Rotational deformity from gluteal muscles
Treatment
- Anatomical reduction
- Usually fixed with two screws to control rotation
AVN Risk
- Lower than Type II
Type IV – Intertrochanteric Fracture
Features
- Extracapsular injury
- Lowest AVN risk
- Good healing potential
Treatment
| Stability | Treatment |
|---|---|
| Stable | Screw fixation |
| Unstable | Plate fixation |
Special Fracture Situations
Combined Femoral Neck and Shaft Fracture
Important Principle
- Fix the femoral neck first
- Then address shaft fracture using:
- Elastic nails
- Spica cast
Pathological Fracture
Common Cause
- Unicameral bone cyst
Clue
- Fallen fragment sign
Management
- Stabilize fracture first
- Treat cyst later
Stress Fracture
- Requires early diagnosis and treatment
- Prevents progression to complete fracture
Avascular Necrosis (AVN)
Avascular necrosis of femoral head
Incidence
- Approximately 30–40% overall
Major Causes
- Initial trauma
- Blood supply disruption
- Increased intracapsular pressure from hematoma
Capsulotomy and Decompression
Important Principle
Capsular decompression and hematoma evacuation may reduce AVN risk.
Evidence Trend
| Treatment | AVN Rate |
|---|---|
| Without decompression | Up to 40% |
| With capsulotomy | Less than 10% |
Core Principles of Treatment
1. Urgent Management
- Same-day surgery preferred
2. Anatomical Reduction
- Closed reduction first
- Open reduction if necessary
3. Stable Internal Fixation
Options include:
- Cannulated screws
- Plates
4. Capsular Decompression
- Helps reduce AVN risk
Major Complications
1. Avascular Necrosis
- Segmental or complete femoral head involvement
- May progress to collapse
2. Coxa Vara
Caused by:
- Poor fixation
- Muscle deforming forces
- Cast treatment alone
3. Non-union
Important Radiological Sign
- “Windshield wiper sign” indicating loosening screws
4. Growth Arrest
- Neck shortening
- Altered hip biomechanics
5. Stress Fracture After Implant Removal
- Protected weight-bearing recommended after implant removal
High-Yield Exam Pearls
- Pediatric hip fractures are rare but dangerous
- Delbet Type I has the highest AVN risk
- Delbet Type IV has the best prognosis
- Urgent reduction and fixation are essential
- Capsulotomy may reduce AVN risk
- In combined injuries, fix the neck first
- Avoid superior screw placement to preserve blood supply
- Rotational deformities do not remodel well

Leave a Reply