Courtesy: Amr Abdelgawad, Maimonaides Medical Centre, NY, USA
Posterolateral Approach to the Ankle
- Commonly used for ORIF of posterior malleolus fractures.
- Interval: between peroneal tendons (lateral) and flexor hallucis longus (medial).
- Flexor hallucis longus muscle extends distally close to the ankle (“beef to heel” characteristic).
- Structure at risk: Sural nerve.
- Small saphenous vein lies medial to the sural nerve.
- To protect the nerve, retract the vein laterally.
Lateral Approach to the Fibula
- Used for fixation of lateral malleolus fractures.
- Structure at risk: Superficial peroneal nerve.
- Nerve becomes superficial approximately 12 cm proximal to the tip of the distal fibula.
- Care is required during dissection around this level.
Anterior Approach to the Ankle
- Structure most at risk: Medial dorsal cutaneous branch of the superficial peroneal nerve.
- Important during open ankle surgery.
- Nerve injury may cause dorsal foot sensory deficits.
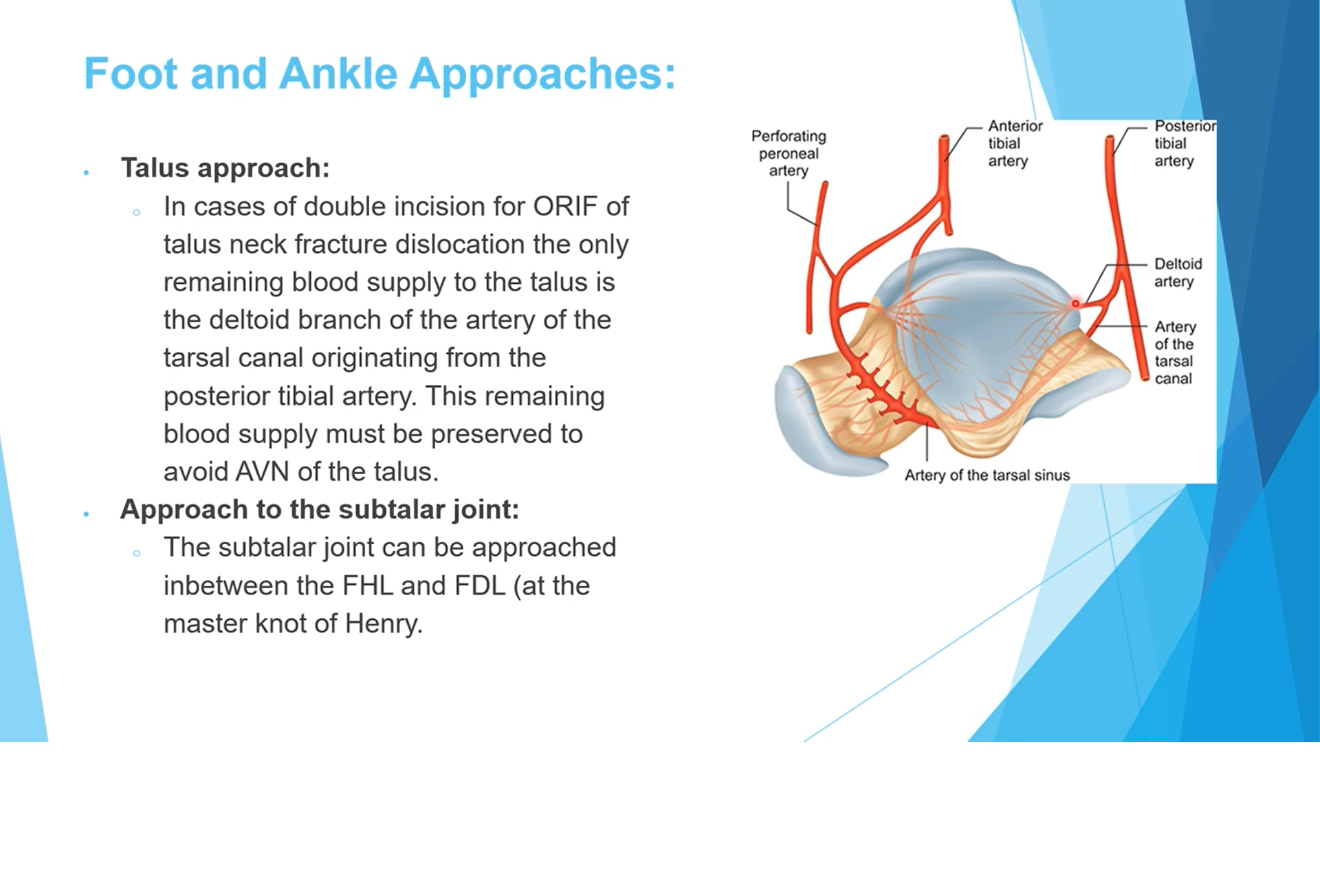
Talus Fracture Surgical Considerations
- Double incision approaches risk disruption of talar blood supply.
- Deltoid branch of the artery of the tarsal canal may remain the only blood supply.
- Preservation of deltoid branches is critical to avoid avascular necrosis.
Master Knot of Henry
- Crossing point of flexor hallucis longus (FHL) and flexor digitorum longus (FDL).
- Occurs near the level of the subtalar joint.
- FHL passes deep to FDL.
- Important surgical landmark in medial foot approaches.
Extensile Lateral Approach for Calcaneus
- Used for calcaneal fracture fixation.
- Provides excellent exposure of the calcaneus.
- Requires elevation of a lateral skin flap.
- Main blood supply of the flap: Lateral calcaneal artery.
- Artery located approximately 1.5 cm anterior to Achilles tendon.
- Vertical incision placed about 0.5 cm from Achilles tendon to avoid vascular injury.
Ankle Arthroscopy Portals
- Anteromedial portal: medial to tibialis anterior tendon.
- Structures at risk: saphenous nerve and saphenous vein.
- Anterolateral portal: lateral to peroneus tertius tendon.
- Structures at risk: superficial peroneal nerve or intermediate dorsal cutaneous branch.
- Posterolateral portal: lateral to Achilles tendon.
- Structures at risk: sural nerve and small saphenous vein.
- Most commonly injured nerve during ankle arthroscopy: intermediate dorsal cutaneous branch.
Anterior Tibial Artery and Deep Peroneal Nerve Relationship
- In the lower leg: anterior tibial artery lies medial to the deep peroneal nerve.
- At ankle level the artery passes beneath extensor retinaculum.
- Foot relationship (medial ? lateral): tibialis anterior ? extensor hallucis longus ? artery & nerve ? extensor digitorum longus.
Intrinsic Muscles of the Foot
- Function similar to intrinsic muscles of the hand.
- Flex metatarsophalangeal joints.
- Extend interphalangeal joints.
- Weakness results in claw toe deformity: MTP extension with IP flexion.
Compartments of the Foot
- Total of nine compartments.
- Four interosseous compartments.
- Medial compartment.
- Lateral compartment.
- Two central compartments (superficial and deep/adductor).
- Calcaneal compartment.
- There is no dorsal compartment.
Syndesmosis Ligaments
- Interosseous ligament between tibia and fibula.
- Anterior inferior tibiofibular ligament (AITFL).
- Posterior inferior tibiofibular ligament (PITFL).
- AITFL avulsion fracture produces Tillaux fracture.
Flexor Hallucis Longus Anatomy
- Runs lateral to the posteromedial tubercle of the talus.
- Passes in a groove behind the talus.
- Turns under the sustentaculum tali.
- Long calcaneal screws may irritate the FHL tendon.
- Crosses flexor digitorum longus at the Master Knot of Henry.
Peroneal Tendons
- Peroneus brevis lies deeper and closer to the fibula.
- Mnemonic: “Brevis is by the Bone”.
- Peroneus longus lies more superficial.
- Peroneal tubercle separates the tendons at the calcaneus.
- Peroneus brevis passes superior/anterior to the tubercle.
- Peroneus longus passes inferior/plantar to the tubercle.
Functions of Peroneal Muscles
- Peroneus brevis: foot eversion.
- Peroneus longus: eversion and plantarflexion of the first ray.
- Peroneus longus contributes to maintenance of the longitudinal arch.
Muscle Antagonists in Foot Mechanics
- Posterior tibial muscle (inversion) vs peroneus brevis (eversion).
- Tibialis anterior (inversion and dorsiflexion) vs peroneus longus (eversion and plantarflexion of first ray).
- Important in cavus foot pathology.
Lisfranc Ligament
- Connects medial cuneiform to base of second metatarsal.
- Key stabilizer of the tarsometatarsal joint.
- Injury results in Lisfranc fracture-dislocation.
Spring Ligament (Plantar Calcaneonavicular Ligament)
- Runs from calcaneus to navicular.
- Supports the talar head and talonavicular joint.
- Prevents collapse of the medial arch.
- Injury associated with posterior tibial tendon dysfunction.
- Important in adult acquired flatfoot deformity.
Lateral Ankle Ligaments
- Anterior talofibular ligament (ATFL) most commonly injured.
- ATFL stressed during inversion and plantarflexion.
- Calcaneofibular ligament stressed during inversion and dorsiflexion.
Hallux Sesamoids
- Two sesamoids: medial (tibial) and lateral (fibular).
- Embedded in the tendons of flexor hallucis brevis.
- Flexor hallucis longus tendon runs between them.
- Excision of medial sesamoid may cause hallux valgus.
- Excision of lateral sesamoid may cause hallux varus.
- Removal of both sesamoids may produce cock?up deformity.
- Plantar plate attaches to the base of the proximal phalanx.
Blood Supply of the Talus
- Three main sources: artery of tarsal canal, artery of sinus tarsi, and deltoid branch.
- Tarsal canal artery from posterior tibial artery supplies most of talar body.
- Deltoid branch supplies medial talar body.
- Sinus tarsi artery from anastomosis of anterior tibial and perforating peroneal arteries.
- Sinus tarsi artery supplies talar head and neck.
- Deltoid branch may be the only remaining blood supply after talar fractures.


Leave a Reply