Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Differential Diagnosis of Trigger Finger
Introduction
Trigger finger is a common condition caused by stenosing tenosynovitis at the A1 pulley, resulting in painful locking or catching of the finger during movement.
However, several other conditions can mimic trigger finger and should be differentiated carefully during clinical evaluation.
1. Lumbrical Plus Finger
Definition
Lumbrical plus finger is a condition characterized by paradoxical extension of the finger during attempted flexion.
Mechanism
The condition occurs due to abnormal pull of the lumbrical muscle, often resulting from disruption or shortening of the flexor digitorum profundus (FDP) tendon mechanism.
Causes
Common causes include:
- FDP tendon injury
- Tendon shortening
- Distal finger amputation
Clinical Features
Characteristic Finding
- When the patient attempts to make a fist, the affected finger extends instead of flexing
This phenomenon is called:
- Paradoxical extension
Key Point
Unlike true trigger finger, the pathology is related to tendon imbalance rather than A1 pulley stenosis.
2. PIP Joint Pathology and Paradoxical Extension
Overview
Pathology involving the proximal interphalangeal (PIP) joint can produce abnormal tendon mechanics that mimic triggering.
Clinical Features
Patients may present with:
- Difficulty coordinating finger flexion
- Catching or abnormal finger movement
- Apparent triggering sensation
Important Point
This condition should be differentiated from true stenosing tenosynovitis because the underlying problem arises from joint or tendon imbalance rather than pulley constriction.
3. Sagittal Band Injury (Extensor Hood Injury)
Definition
Sagittal band injury involves disruption of the sagittal band, leading to instability or subluxation of the extensor tendon.
Common Site
- Metacarpophalangeal (MCP) joint
- Most commonly affects the middle finger
Mechanism
Damage to the sagittal band allows the extensor tendon to subluxate during finger motion.
Clinical Features
Patients may complain of:
- Snapping sensation
- Triggering-like movement
- Pain over the MCP joint
On examination:
- The extensor tendon may dislocate during flexion and extension
Key Point
Although it may resemble trigger finger clinically, the pathology is located on the extensor side of the finger rather than the flexor pulley system.
4. True Trigger Finger
Pathophysiology
True trigger finger is caused by stenosis at the A1 pulley, leading to impaired gliding of the flexor tendon.
Clinical Features
Typical findings include:
- Pain over the A1 pulley
- Finger locking in flexion
- Triggering during motion
- Requirement for passive extension in severe cases
Quick Clinical Differentiation
| Condition | Key Feature | Site of Pathology |
|---|---|---|
| Trigger finger | Locking in flexion | Flexor tendon at A1 pulley |
| Lumbrical plus finger | Extension during attempted flexion | Lumbrical–FDP imbalance |
| Sagittal band injury | Snapping at MCP joint | Extensor tendon mechanism |
| PIP-related pathology | Abnormal coordinated motion | Joint or tendon imbalance |
Key Take-Home Points
- Trigger finger is caused by stenosing tenosynovitis at the A1 pulley.
- Lumbrical plus finger produces paradoxical extension during attempted fist formation.
- Sagittal band injuries involve extensor tendon instability at the MCP joint.
- PIP joint pathology may mimic triggering because of altered tendon mechanics.
- Careful clinical examination helps distinguish these conditions and guides appropriate treatment.

Related Posts
 Paediatric Elbow Dislocation and Differential Diagnosis
Paediatric Elbow Dislocation and Differential DiagnosisCourtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA Basic Facts Commonly seen in…
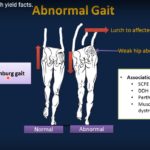 The Limping child and Differential Diagnosis
The Limping child and Differential DiagnosisCourtesy: Osama Naga, Texas Tech University Health Sciences, El Paso, Texas, USA
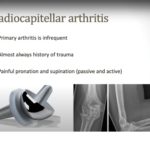 Differential Diagnosis of Lateral Elbow Pain
Differential Diagnosis of Lateral Elbow PainCourtesy: Dr Michelle Ruiz Suares, President Mexico Shoulder and Elbow Society, Mexico city, Mexico …
Leave a Reply