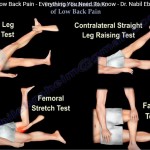
Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Complicated Low Back Pain – Clinical Overview
Introduction
Low back pain is one of the most common clinical complaints encountered in medical practice.
Most cases are:
- Non-specific
- Self-limiting
- Multifactorial
However, some patients present with red flags or serious underlying pathology that require urgent evaluation and treatment.
Epidemiology
- Approximately 85% of low back pain cases have no clearly identifiable specific cause.
- Nearly 95% improve within 3 months.
- Pain is often:
- Multifactorial
- Non-organic
- Referred from non-spinal structures
Referred Pain Sources
Low back pain may originate outside the spine.
Important causes include:
- Hip joint pathology
- Buttock pathology
- Sacroiliac joint disorders
- Abdominal aortic aneurysm
- Renal stones
- Pancreatitis
- Pelvic pathology
- Acute myocardial infarction
Always exclude non-spinal causes before attributing symptoms solely to the lumbar spine.
Red Flag Signs
Presence of red flags requires urgent evaluation.
Important red flags include:
- Significant trauma
- History of malignancy
- Fever
- Chills
- Unexplained weight loss
- Progressive neurological deficit
- Bladder dysfunction
- Bowel dysfunction
Serious Conditions
Cauda Equina Syndrome
Clinical Features
Typical findings include:
- Severe back pain greater than leg pain
- Saddle anesthesia
- Bladder dysfunction
- Bowel dysfunction
- Bilateral lower limb symptoms
Management
This is a surgical emergency.
Required steps:
- Emergency MRI
- Urgent decompression surgery
Delayed treatment may result in permanent neurological deficit.
Progressive Neurological Deficit
Patients with worsening neurological symptoms require evaluation of the entire spine.
Assessment should include:
- Lumbar spine
- Thoracic spine
- Cervical spine
If MRI is contraindicated:
- CT myelography may be used
Gait Disturbance with Back Pain
Gait disturbance in a patient with back pain should raise suspicion for cervical myelopathy.
Always examine for:
- Upper motor neuron signs
- Hyperreflexia
- Hoffmann sign
- Babinski sign
- Spasticity
MRI of the cervical spine may be required.
Special Clinical Situations
Smoking
Smoking negatively affects spinal health by:
- Reducing disc nutrition
- Impairing fusion healing
- Increasing surgical failure rates
Smokers generally have poorer surgical outcomes.
Depression
Depression is an independent predictor of poor outcomes after spinal surgery.
Psychological assessment is important in chronic low back pain patients.
Ankylosing Spondylitis
Patients with ankylosing spondylitis are at risk for:
- Occult spinal fractures
- Neurological deficit
Minor trauma may cause unstable fractures.
Imaging should include:
- CT scan
- MRI if needed
Osteoporotic Compression Fracture
Clinical Features
Elderly patients with acute severe back pain should be evaluated for compression fractures.
Investigations
Important investigations include:
- Plain X-ray
- DEXA scan
Management
Treatment options include:
- Bracing
- Osteoporosis management
- Pain control
- Surgery in selected cases
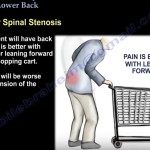
Neurogenic Claudication
Lumbar Spinal Stenosis
Neurogenic claudication is a classic manifestation of lumbar spinal stenosis.
Clinical Features
Symptoms include:
- Back pain
- Leg heaviness
- Cramping
- Weakness during walking
Symptoms worsen with:
- Standing
- Walking
Symptoms improve with:
- Sitting
- Forward bending
Shopping Cart Sign
Patients often feel relief while leaning forward on a shopping cart.
This is a classic feature of lumbar spinal stenosis.
Differentiation from Vascular Claudication
Vascular claudication may coexist with spinal stenosis.
Important distinctions:
| Feature | Neurogenic Claudication | Vascular Claudication |
|---|---|---|
| Worse with | Standing/walking | Walking |
| Relief | Sitting/flexion | Rest |
| Pulses | Usually normal | Reduced |
| Bicycle test | Often tolerated | Pain persists |
Vascular assessment may be necessary.
MRI – Important Concept
MRI findings must always correlate with clinical symptoms.
Important point:
- MRI abnormalities are common in asymptomatic individuals.
Never treat MRI findings alone.
Factors Associated with Poor Surgical Outcome
Poor outcomes are more common in patients with:
- Workers’ compensation claims
- Smoking
- Depression
- Non-specific back pain
Careful patient selection is essential.
Key Clinical Pearls
- Most low back pain is non-specific and self-limiting.
- Always evaluate for red flags.
- Bladder or bowel dysfunction suggests cauda equina syndrome.
- Gait disturbance should raise suspicion for cervical myelopathy.
- MRI findings require clinical correlation.
- Neurogenic claudication improves with sitting or forward flexion.
- Always consider non-spinal causes of back pain.

Leave a Reply