Courtesy: Dave Lee, Ashok Shyam, Ortho TV
Arthroscopic Management of Medial Meniscus Tear with Parameniscal Cyst
Patient Presentation
-
A female patient in her thirties presented with right knee pain for three years.
-
Symptoms began after a fall from a motorbike.
-
Complaints included:
-
Pain during standing and walking
-
Pain while climbing stairs
-
Night pain
-
-
The patient did not report instability of the knee.
Clinical Examination
Range of Motion
-
No fixed flexion deformity was observed.
-
No hyperextension was present.
-
The knee demonstrated full painless motion from full extension to approximately one hundred thirty five degrees of flexion.
Joint Examination
-
No joint effusion was noted.
-
Patellar tracking and patellar glide were normal.
Palpation
-
Marked tenderness along the medial joint line, particularly in the posterior region.
Ligament Stability Tests
-
Anterior cruciate ligament testing was stable.
-
Posterior cruciate ligament testing was stable.
-
Varus and valgus stress tests were negative.
Overall, the knee was stable without evidence of ligament injury.
Gait
-
The patient walked without an antalgic gait.
Radiographic Evaluation
Long Leg Alignment Radiograph
-
Mechanical axis passed slightly medial to the medial tibial spine.
-
Overall limb alignment was near neutral.
Standard Knee Radiographs
-
Medial and lateral joint spaces were preserved.
-
No significant degenerative changes were identified.
Magnetic Resonance Imaging Findings
Magnetic resonance imaging demonstrated:
-
A horizontal tear of the medial meniscus extending from the posterior horn to the mid portion of the meniscus.
-
A parameniscal cyst associated with the medial meniscus.
-
Degenerative changes within the meniscus.
The cyst was seen adjacent to the tear, suggesting fluid extrusion through the meniscal defect.
Diagnosis
The patient was diagnosed with:
-
Horizontal tear of the medial meniscus
-
Associated parameniscal cyst
Surgical Treatment Plan
The planned arthroscopic procedure included:
-
Decompression of the parameniscal cyst
-
Repair of the horizontal medial meniscus tear
-
Augmentation of the repair using arthroscopic sutures
The goal of surgery was to preserve the meniscus and restore joint stability while relieving symptoms caused by the cyst.
Arthroscopic Findings
During arthroscopy, the intra-articular findings differed slightly from the preoperative imaging.
Observations included:
-
A large flap tear of the medial meniscus extending from the body to the posterior horn.
-
The tear involved both the superior and inferior meniscal leaflets.
-
Degenerative changes were present in the posterior horn region.
The tear configuration resembled a long flap component rather than a simple horizontal cleavage tear.
Surgical Technique
Initial Preparation
-
The tear edges were first freshened using a shaver.
-
The surgeon then identified the tract connecting the meniscal tear to the parameniscal cyst.
Cyst Decompression
-
The cyst was decompressed by accessing it from the joint side.
-
Decompression allowed the cystic contents to drain into the joint cavity.
Meniscal Bed Preparation
-
The posterior horn region was carefully debrided and rasped to create a vascular healing environment.
-
Care was taken near the meniscal root.
Decision Between Repair and Resection
The surgeon considered two options:
-
Partial resection of the unstable flap
-
Meniscal repair
Factors influencing the decision included:
-
Patient age
-
Tear configuration
-
Desire to preserve meniscal tissue
Ultimately, meniscal repair was chosen.
Meniscal Repair Technique
Initial Stabilization
-
The tear was first stabilized using all-inside sutures.
Additional Repair
-
Because the tear extended into the body of the meniscus, inside-out suturing techniques were subsequently used.
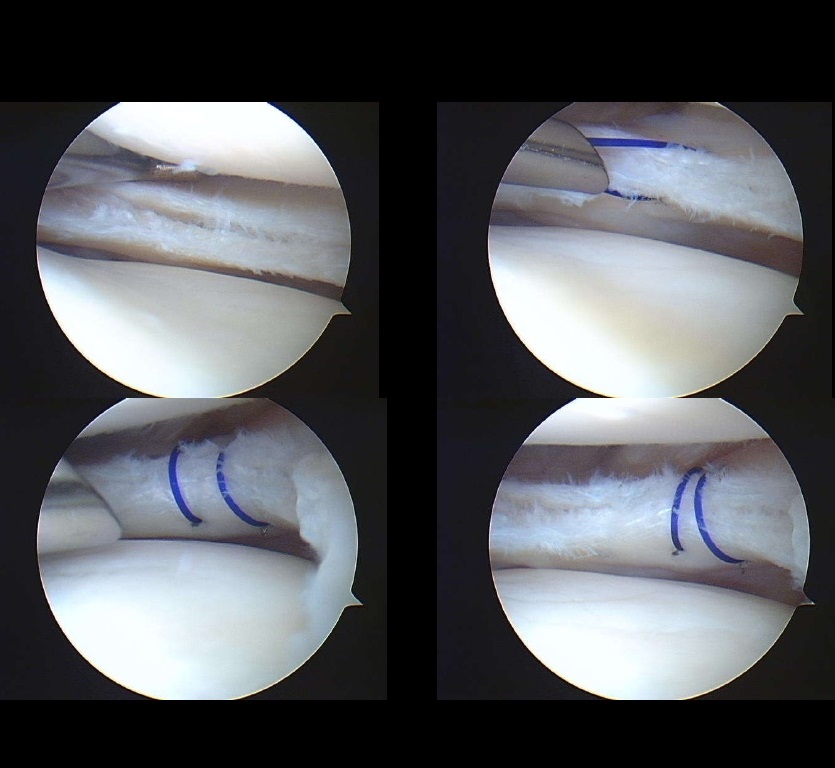
Inside-Out Suturing
-
Multiple sutures were placed through the meniscus from inside the joint outward through the capsule.
-
Approximately four sutures were placed to stabilize the tear.
Advantages of Inside-Out Technique
-
Lower failure rates compared with all-inside devices in certain tear patterns
-
Lower cost
-
Less meniscal tissue damage
-
Greater flexibility in suture placement
Inferior Leaflet Stabilization
-
Additional sutures were placed to capture the inferior leaflet of the meniscal tear, which had been mobile.
This helped restore the anatomical relationship of the meniscal layers.
Biological Augmentation
After completing the repair, additional steps were planned to improve healing.
These included:
-
Microfracture of the intercondylar notch to release marrow elements
-
Consideration of biological augmentation techniques to enhance healing
Meniscal Repair Considerations
Differences Between Medial and Lateral Meniscus Healing
Healing potential differs between the medial and lateral meniscus.
Lateral Meniscus
-
Better vascular supply
-
Higher healing potential
-
Preservation strongly recommended
Medial Meniscus
-
Lower vascularity
-
Higher failure rates after repair
-
Degenerative tears may have limited healing potential
Clinical Implications
Although repair of medial meniscal tears may fail in some cases, meniscal preservation remains desirable because:
-
Meniscal loss increases the risk of osteoarthritis.
-
Meniscal tissue contributes to load distribution and joint stability.
Surgical Technical Tips
Important technical considerations during meniscal repair include:
-
Adequate visualization of the medial compartment
-
Medial collateral ligament pie-crusting if necessary to improve access
-
Careful placement of sutures using appropriate cannulas
-
Protection of surrounding structures during inside-out suturing
Postoperative Assessment
Following repair:
-
The meniscus appeared stable on probing.
-
Sutures secured both superior and inferior meniscal layers.
The procedure concluded after confirming adequate fixation.
Key Points
-
Horizontal medial meniscus tears can be associated with parameniscal cysts.
-
Arthroscopic decompression of the cyst combined with meniscal repair is an effective treatment strategy.
-
Inside-out suturing techniques remain a reliable method for complex meniscal repairs.
-
Meniscal preservation is preferred whenever possible to protect long-term knee joint health.
Related Posts
 Meniscus Repair
Meniscus RepairCourtesy: Dr Dinshaw Pardiwala, Ashok Shyam, Ortho TV Practical Considerations in Meniscus Repair Introduction Meniscus…
 Cartilage Repair of Foot and Ankle
Cartilage Repair of Foot and AnkleCourtesy: Francesca Vannini, Rizzoli Orthopaedic Institute, Bologna, Italy
 Cartilage repair for the Knee Joint
Cartilage repair for the Knee Joint? Courtesy: Christopher McCrum, Assistant Professor, UT SouthWestern, Dallas, Texas, USA Articular Cartilage Structure Basic…
Leave a Reply