Courtesy: Prof Nabil Ebraheim, University of Toledo,Ohio, USA
Chondroblastoma: Key Features and Management
Overview
- Chondroblastoma is a benign but locally aggressive cartilage forming tumor.
- It most commonly occurs in adolescents and young adults.
- The tumor occurs more frequently in males and typically affects skeletally immature patients.
Common Locations
- The lesion typically arises in the epiphysis of long bones.
- The distal femur and proximal tibia are common sites, with most cases occurring around the knee.
- Other frequent sites include the proximal humerus, proximal femur, and calcaneus.
Clinical Presentation
- Patients often present with localized pain.
- Because the tumor is close to the joint, joint related symptoms may occur.
- In some cases, the lesion may extend across the growth plate.
- Rarely, pulmonary metastasis may occur.
Radiological Features
- Radiographs show a lytic epiphyseal lesion with a well defined sclerotic margin.
- Matrix calcification may be present.
- Magnetic resonance imaging often demonstrates surrounding bone marrow and soft tissue edema.
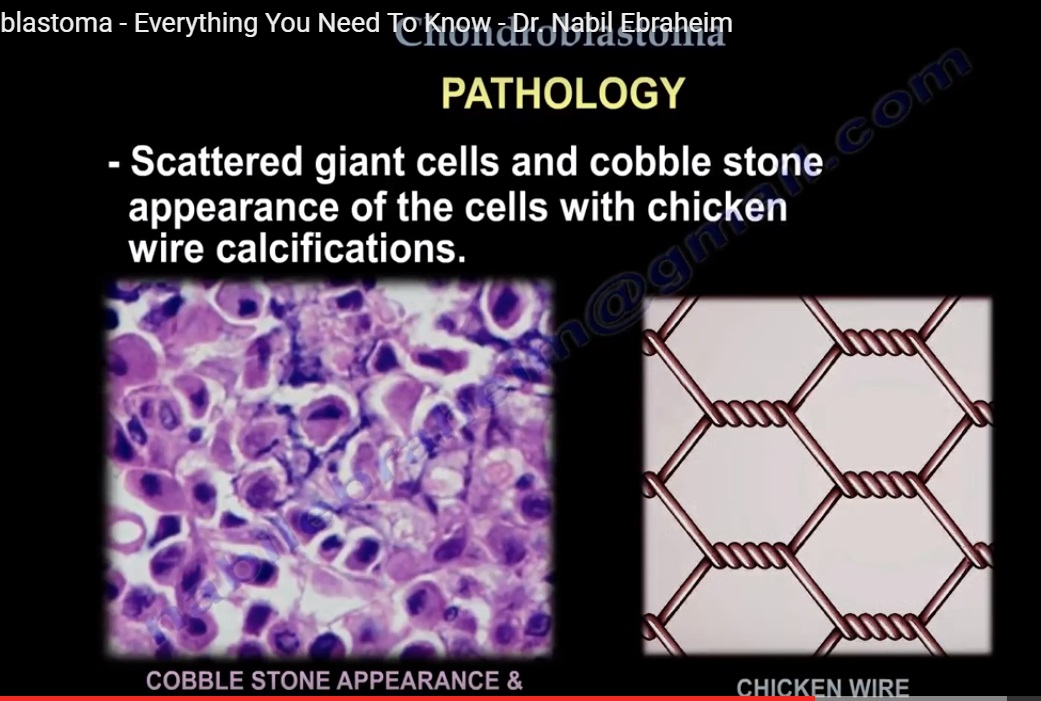
Histopathology
- The tumor consists of polygonal chondroblasts with well defined cytoplasmic borders.
- Nuclei often show longitudinal grooves, producing a coffee bean appearance.
- Scattered multinucleated giant cells may be present.
- Characteristic chicken wire calcification may be seen.
- Some lesions may contain secondary aneurysmal bone cyst components.
Differential Diagnosis
- Clear cell chondrosarcoma, which occurs in older patients and shows more aggressive histology.
- Giant cell tumor, which usually occurs after skeletal maturity and has uniform stromal cells.
- Brodie abscess, which may mimic the lesion clinically and radiologically.
Immunohistochemistry
- Chondroblastoma typically shows positivity for S100 protein, helping distinguish it from giant cell tumor.
Management
- Treatment typically involves intralesional curettage with bone grafting.
- Adjuvant treatments such as phenol or liquid nitrogen may be used in selected cases.
Prognosis
- The recurrence rate is generally less than ten percent with appropriate treatment.
Summary
- Chondroblastoma is a benign epiphyseal tumor with characteristic clinical, radiological, and pathological features.
Early diagnosis and appropriate surgical treatment result in good outcomes
Introduction
• Benign, aggressive, cartilage tumour.
• More common in epiphyseal location.
• Occurs more in males.
• More prevalent in age group 10-25 years.
• Occurs more in skeletal immature persons.
DIFFERENTIAL DIAGNOSIS
OTHER EPIPHYSEAL TUMOURS
1. Clear cell chondrosarcoma
• Epiphyseal lesion
• Occurs in older age group
• More aggressive histological pattern
• Presence of large cells with central nuclei.
• Occurs in proximal humerus and proximal femur.
2. Giant cell tumour
• Occurs in older age group.
• Has uniform cells.
• Nuclei of the stroma is similar to the nuclei of the giant cells .
3. Osteomyelitis
• Brodie’s abscess
WHERE DOES CHONDROBLASTOMA COMMONLY OCCUR?
• Common location- distal femur, proximal tibia, proximal humerus
• 30% of chondroblastoma occurs around the knee followed by the proximal humerus, proximal femur and the calcaneum.
ON EXAMINATION:
• Painful
• Tumors abouts the joint, may create joint symptoms and may also cross the physes.
• 1% of these tumours metastasis to the lung.
RADIOLOGY
1. Lytic epiphyseal lesion with a sclerotic rim.
2. Sharp, well-defined borders.
3. Calcification maybe present in the matrix.
4. MRI may show extensive surrounding edema
PATHOLOGY
• Scattered giant cells and cobblestone appearance of cells with chicken wire calcification.
• 1/3 rd of the lesions may have an aneurysm bone cyst(ABC)
• The lesion is chondroid with polygonal cells.
• Lesion has a defined cytoplasm border and an oval shaped nuclei with a prominent longitudinal groove(coffee beam appearance of the nuclei)
• Chondroblasts can be distinguished from giant cell tumours by staining for the S100 protein, chondroblastoma will be reactive.
TREATMENT
1. Intralesional curettage and bone graft.
2. The recurrence rate is less than 10%.
3. Some surgeons may use adjuvant such as phenol or liquid nitrogen.

Leave a Reply