Courtesy: Sree Metikala MD, Assitant Professor, Virginia C University, Virginia, USA
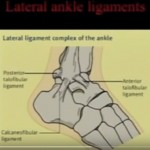
Functional Anatomy of the Lateral Ligament Complex
Components
1. Anterior Talofibular Ligament (ATFL)
- Weakest ligament
- Most commonly injured
- Tight in plantarflexion
2. Calcaneofibular Ligament (CFL)
- Stronger than ATFL
- Stabilizes:
- Ankle joint
- Subtalar joint
- Tight in dorsiflexion
3. Posterior Talofibular Ligament (PTFL)
- Strongest ligament
- Rarely injured
- Usually involved only in ankle dislocation
Important Distinction
- Lateral ligaments — syndesmotic ligaments (proximal)
Acute Ankle Sprain: Treatment Options
Available Options
- Cast immobilization ( 4 weeks)
- Boot immobilization
- Brace + Early functional rehabilitation (preferred)
- Surgery (rare; e.g., unstable avulsion fractures)
Evidence-Based Conclusion
Early mobilization is superior:
- Faster return to activity
- Lower recurrence rates
Functional Rehabilitation (Early Mobilization)
Phase 1: Protection (First Week)
- Brace or boot
- Controlled weight-bearing
Phase 2: Rehabilitation
Exercises
- Range of motion
- Stretching
- Peroneal strengthening
- Proprioception training
Key Advantages
- Improves neuromuscular control
- Faster recovery
- Prevents chronic instability
Persistent Pain After Ankle Sprain
Common Causes
- Syndesmotic injury
- Deltoid ligament injury
- Peroneal tendon pathology
- Superior peroneal retinaculum injury
- Osteochondral lesions
- Superficial peroneal nerve neuropraxia
Important Clinical Note
Early treatment of neuropathic pain (e.g., gabapentin/pregabalin)
May help prevent CRPS
Chronic Ankle Instability
Definition
Triad of:
- Recurrent sprains
- Pain
- Giving way
Types
1. Mechanical Instability
- True ligament laxity
- Positive stress tests
2. Functional Instability
- Subjective instability
- Poor proprioception
- No ligament laxity
Clinical Examination
Assessment Positions
- Standing
- Walking
- Single heel rise
- Sitting
Stress Tests
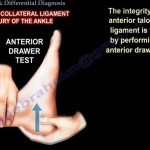
Anterior Drawer Test
- Tests ATFL
- Performed in plantarflexion
Talar Tilt Test
- Tests ATFL + CFL
- Performed in dorsiflexion
Grading of Ankle Sprains
| Grade | Injury |
|---|---|
| Grade I | Partial ATFL tear |
| Grade II | Complete ATFL tear |
| Grade III | ATFL + CFL tear |
Clinical Challenge
- Difficult to assess acutely due to:
- Pain
- Muscle spasm
Non-Operative Management (Chronic Instability)
First-Line
Structured rehabilitation (minimum 3 months)
Components
- Stretching
- Bracing
- Peroneal strengthening
- Proprioception training
- Lateral heel wedge (if needed)
Indications for Surgery
- Failure of adequate rehabilitation
- Persistent instability
Surgical Options
1. Non-Anatomic Reconstruction (Tenodesis)
- Uses tendon graft (e.g., peroneus brevis)
Disadvantages
- Stiffness
- Altered biomechanics
2. Anatomic Repair (Preferred)
Broström Procedure
- Direct ligament repair
Modified Broström (Gold Standard)
- Augmented repair
- Uses suture anchors
Technique
- “Triple breasting” of ligament
3. Ligament Reconstruction
Indications
- Chronic attenuation
- Revision cases
Grafts
- Autograft
- Allograft
Role of Arthroscopy
Indications
- Osteochondral lesions
- Intra-articular pathology
Advantages
- Faster early recovery
- Minimally invasive
Outcomes
- Comparable long-term to open surgery
Adjunct Procedures
- Osteotomy (for deformity correction)
- Peroneal tendon repair
- Combined arthroscopic procedures
Treatment Algorithm
Acute Sprain
- X-ray – rule out fracture
- Early functional rehabilitation
Chronic Instability
- Structured rehabilitation
If Failure
- MRI evaluation
- Surgical repair/reconstruction
Key Take-Home Points
- ATFL is the most commonly injured ligament
- Early mobilization provides best outcomes
- Persistent pain — evaluate for missed injuries
- Rehabilitation is first-line for instability
- Modified Broström = gold standard surgical treatment


Leave a Reply