Courtesy: Kaye Wilkins, Lynn Staheli , www.global-help.org
Pediatric Ankle Fractures (Distal Tibia & Fibula)
Key Concept
- In children physis is weaker than ligaments
- So injuries occur through growth plate (physeal fractures) rather than ligament tears
- Hence: better called
“Fractures around the ankle in the skeletally immature”
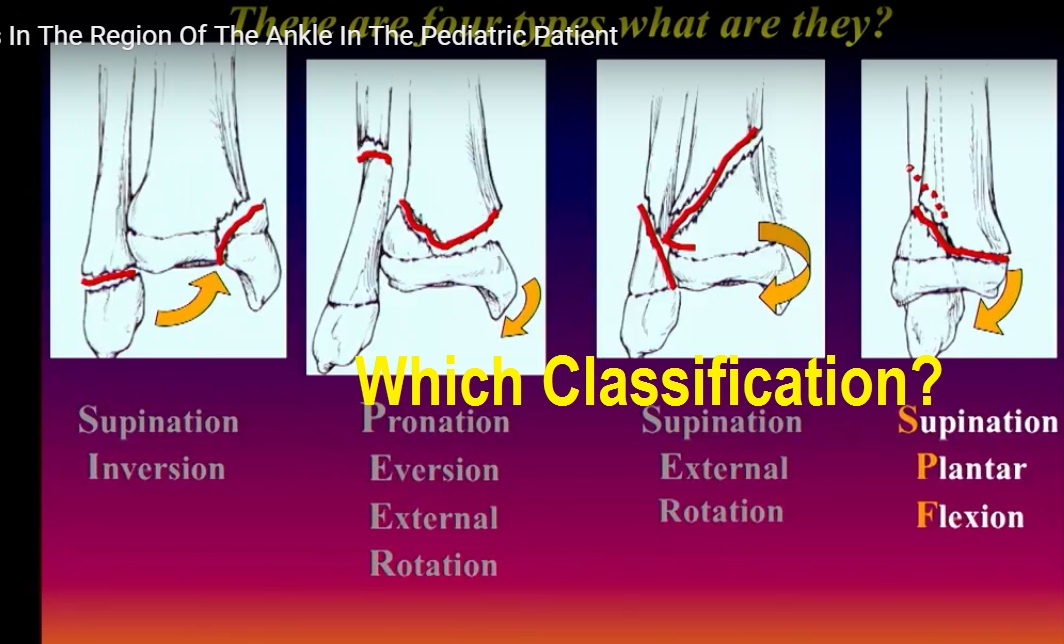
Classification
Not very useful:
- Salter-Harris classification (limited value for ankle decision-making)
Most useful:
Mechanism-based classification (Pediatric counterpart of Lauge-Hansen)
Goals of Classification
- Predict fracture pattern
- Guide treatment
- Predict complications
Main Injury Patterns
Supination–Inversion Injury (Most common)
Stage 1
- Injury: distal fibular physis
- Often undisplaced
- Mimics ankle sprain
Clinical:
- Tenderness over fibular physis (NOT ligaments)
Treatment:
- Functional:
- Air cast / brace
- Early mobilization
Complication:
- Chronic pain due to muscle weakness (immobilization)
Stage 2
- Medial side: compression injury
- Often Salter III/IV medial malleolus
Important:
- Crushing injury high risk of growth arrest
Treatment:
- Anatomical reduction
- Fixation with screw (compression)
- Check joint congruity (arthrogram)
Complications:
- Physeal arrest varus deformity
- Fibular overgrowth
- Ankle incongruity arthritis
2 Pronation–External Rotation Injury
Features:
- Medial: avulsion fracture (tension)
- Lateral: fibular fracture (diaphyseal/metaphyseal)
Deformity:
- Valgus
Treatment:
- Usually closed reduction + cast
- If unstable smooth K-wire (central placement)
Complication:
- Rare growth arrest (usually symmetrical)
Special Issue:
- Periosteal interposition failed reduction
If gap persists OPEN REDUCTION
3 Supination–External Rotation Injury
Sequence:
- Tibia fails first
- Then fibula
Deformity:
- External rotation
Treatment:
- Closed reduction (internal rotation)
- Fix if unstable
Complication:
- Residual external rotation deformity
4 Supination–Plantar Flexion Injury
Features:
- Posterior tibial fracture (avulsion)
- Fibular greenstick
Treatment:
- Reduction with:
- Knee flexion
- Ankle plantarflexion
- Fix if unstable
Special Adolescent Injuries
5 Juvenile Tillaux Fracture
- Avulsion of anterolateral distal tibia
- Caused by:
pull of anterior inferior tibiofibular ligament
Occurs because:
- Medial physis closed
- Lateral still open
Treatment:
- Screw fixation (mandatory if displaced)
Complication:
- Articular incongruity ? arthritis
6 Triplane Fracture
Involves 3 planes:
- Sagittal (epiphysis)
- Coronal (metaphysis)
- Transverse (physis)
Diagnosis:
- X-ray + CT scan (essential)
Treatment:
- Closed/open reduction
- Screw fixation in correct planes
Complication:
- Rare growth arrest (growth nearly complete)
Important Clinical Pearls
Always check:
- Mortise view (mandatory)
- Joint congruity
Fibula fracture rule:
If fibula fractured suspect tibial injury
Reduction principles:
- Reverse mechanism of injury
- Achieve:
- Anatomical reduction
- Stable fixation
Follow-up:
- Look for Harris growth arrest lines
- Asymmetry growth arrest
Most Important Complication
Physeal Arrest
Leads to:
- Angular deformity (varus/valgus)
- Limb length discrepancy (less common)
- Ankle arthritis
Management of Growth Arrest
- Fibular epiphysiodesis
- Tibial osteotomy (e.g., opening wedge)
- Bar resection (if early)
Exam Summary Line
Best classification in pediatric ankle fractures = Mechanism-based (supination/pronation patterns), not Salter-Harris

Leave a Reply