Courtesy: Prof Nabil Ebraheim ,University of Toledo, Ohio, USA
Overview
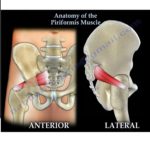
The piriformis muscle is one of the six short lateral rotators of the hip. It occupies a key anatomical position in the deep gluteal region and serves as an important landmark for neurovascular structures exiting the pelvis through the greater sciatic foramen.
Origin
The piriformis muscle arises from:
-
The anterior (pelvic) surface of the sacrum, usually from the second to fourth sacral segments
-
The capsule of the sacroiliac joint
-
The margin of the greater sciatic notch
Because of its origin from the sacrum and sacroiliac joint capsule, there is a recognized association between piriformis syndrome and sacroiliac joint–related pain.
Insertion
-
Inserts onto the superior border of the greater trochanter of the femur
Function
-
Lateral (external) rotation of the hip
-
Abduction of the hip when the hip is flexed
-
Acts as a dynamic stabilizer of the hip joint
Innervation
-
Nerve to piriformis
-
Root values: L5, S1, S2
Relations
Superior Relations
-
Superior gluteal nerve
-
Superior gluteal artery
Inferior Relations
-
Inferior gluteal nerve
-
Inferior gluteal artery
The piriformis muscle effectively divides the greater sciatic foramen into:
-
Suprapiriform foramen
-
Infrapiriform foramen
Relationship of the Sciatic Nerve to the Piriformis Muscle
The sciatic nerve is composed of:
-
Tibial division
-
Common peroneal (fibular) division
These divisions are usually bound together but may separate as they pass the piriformis muscle. Several anatomical variations are described.
Anatomical Variations of the Sciatic Nerve–Piriformis Relationship
Type 1 (Most Common)
-
The entire sciatic nerve passes inferior to the undivided piriformis muscle
Type 2
-
The piriformis muscle is divided
-
The common peroneal division passes between the two heads of the piriformis
-
The tibial division passes below the muscle
Type 3
-
The common peroneal division passes above the undivided piriformis
-
The tibial division passes below the muscle
-
The two divisions appear to “straddle” the piriformis
Type 4 (Rare)
-
The entire sciatic nerve passes through a divided piriformis muscle
Clinical Significance
-
Variations in the relationship between the sciatic nerve and piriformis muscle are important in:
-
Piriformis syndrome
-
Sciatica without spinal pathology
-
Hip surgery and posterior approaches
-
Image-guided injections and nerve blocks
-
-
Hypertrophy, spasm, or inflammation of the piriformis may compress the sciatic nerve, particularly in variant anatomies
Key Take-Home Points
-
Piriformis is a key deep gluteal landmark muscle
-
It externally rotates the hip and abducts the hip in flexion
-
Innervated by L5–S2
-
Closely related to major neurovascular structures
-
Anatomical variations of the sciatic nerve are clinically important and common

Leave a Reply