Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
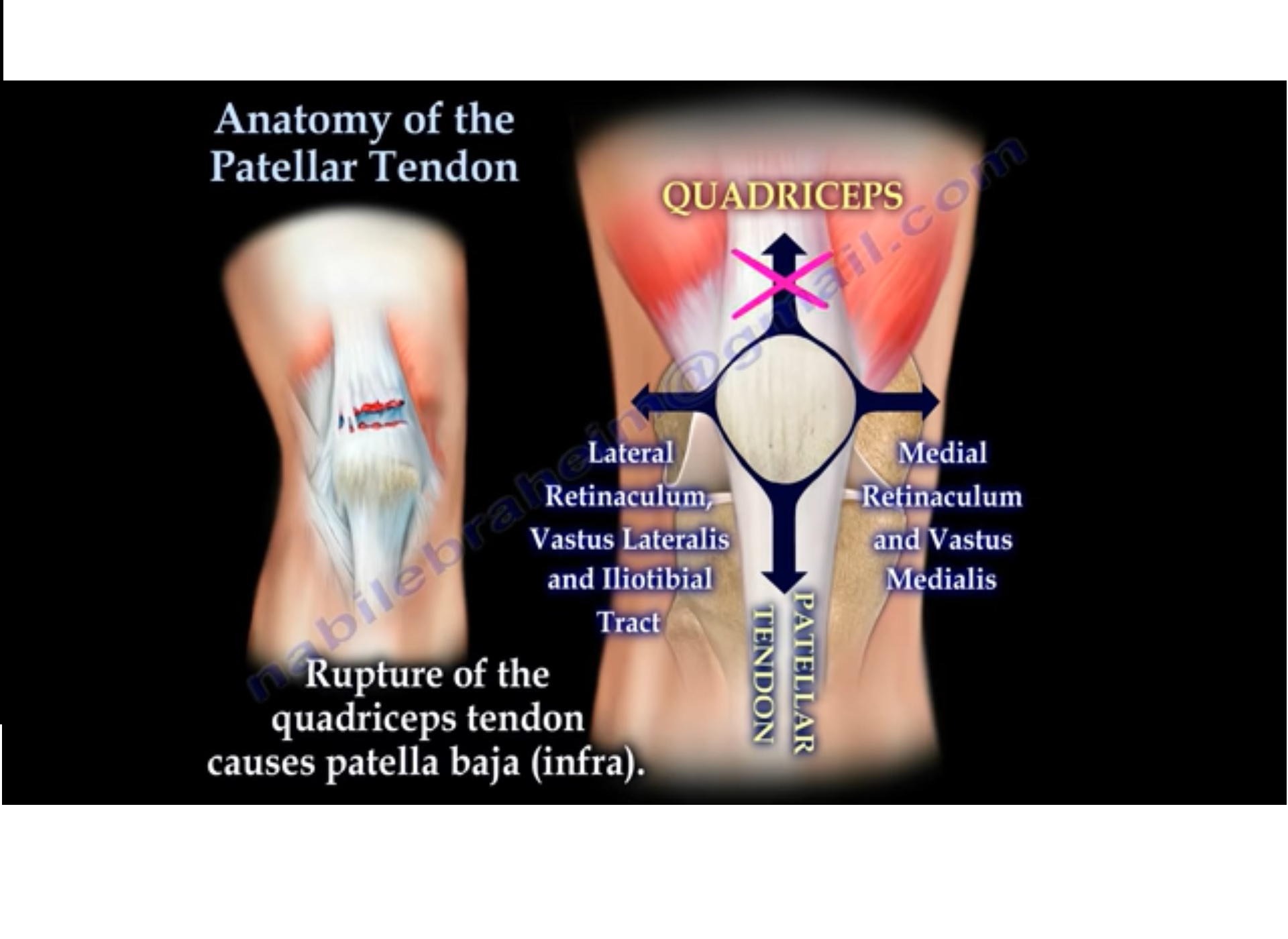
ANATOMY OF PATELLAR TENDON
• The patellar tendon attaches the patella to the top of the tibia.
• The quadriceps muscle is attached superiorly to the patella.
• A small part of the quadriceps tendon then continues over the front of the patella to become the patellar tendon.
• Arterial supply of the patellar tendon.
• The patellar tendon works with the quadriceps to straighten the leg.
• Several bursa are seen around the patella:-
1. Suprapatellar
2. Prepatelllar
3. Infrapatellar
• These bursae allow the knee cap to slide freely underneath the skin while bending and straightening the knee.
• The bursa may become inflamed due to trauma or infection, however bursitis of the knee most commonly occurs in the knee
cap.
• The femoral condyles are covered with the hyaline cartilage and forms the femoral trochlea.
• The patella articulates with the femoral trochlea.
• The patella lies just above the femoral trochlea when the knee is in full extension.
• The patella is classified as a sesamoid bone of the quadriceps tendon with a proximal base and a distal apex (triangular).
• The lateral facet is larger than the medial facet.
• The articular surface of the patella is covered with hyaline cartilage and has two articular facets for the femur.
• The apex, which is the distal part, is nonarticular.
• This area does give attachment to the patellar tendon.
• Patellar tendonitis may develop due to repeated stress being placed on the patellar tendon.
• This condition occurs in athletes from overuse.
• A weakened patellar tendon is more likely to tear and it may become torn where it attached to the kneecap.
• Patellar tendon tears can be either partial or complete.
• When the patellar tendon is ruptured , the quadriceps will pull the patella upward.
• Imaging tests such as X-ray or MRI may be ordered to confirm the presence of a patellar tendon rupture.
• Complete tears can often be identified with X-rays alone.
• MRI shows rupture of the patellar tendon.
• One way to measure patella height is by measuring the BLUMENSAAT’S LINE.
• The knee needs to be flexed at least 30 degrees, then a line can be drawn through the roof of the intercondylar notch and usually touches the tip of the patella.
• The patella moves upward with the patellar tendon rupture(patella alta.)
• Rupture of the patellar tendon causes the patella alta
• Rupture of the quadriceps tendon causes patella baja (infra).
• Lateral dislocation of the patella also seen in “sunrise”view.
• May also cause direct impact injury to the medial patella and lateral femoral condyle.
How long does it take for the patella tendon to repair after a rupture