Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Overview
- The acetabulum is an important component of the hip joint and forms the socket for the femoral head.
- For clinical and surgical purposes, the acetabulum is divided into two structural columns.
- Understanding these columns is essential for interpreting acetabular fractures and planning surgical treatment.
- Several important vessels and nerves are closely related to the acetabulum and may be at risk during trauma or surgical approaches.
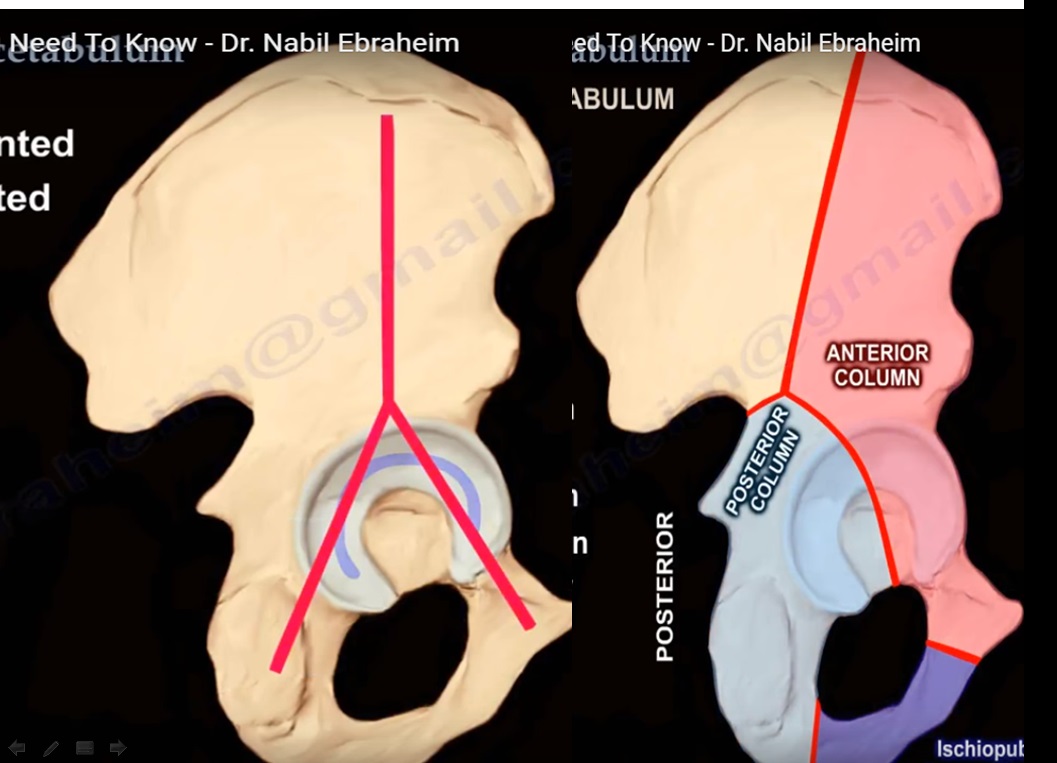
Columns of the Acetabulum
The acetabulum is divided into:
- Anterior column
- Posterior column
These columns form the structural framework of the acetabulum.
Anterior Column
The anterior column consists of:
- Anterior portion of the ilium
- Anterior wall of the acetabulum
- Weight-bearing dome of the acetabulum
- Superior pubic ramus
This column contributes to the anterior and superior structural support of the acetabulum.
Posterior Column
The posterior column extends from:
- Obturator foramen
- Posterior aspect of the acetabular dome
- Greater sciatic notch
This column provides the posterior structural support of the hip socket.
Ischiopubic Ramus
- The ischiopubic ramus is formed by the union of:
- Inferior pubic ramus
- Inferior ramus of the ischium
- It forms the inferior border of the obturator foramen.
Pelvic Structural Orientation
- The pelvis can be conceptually visualized as forming an inverted Y-shaped structure.
- This configuration represents the structural relationship between the anterior and posterior columns of the acetabulum.
Important Vascular Anatomy
Several vessels are closely related to the acetabulum and may be injured in pelvic trauma or during surgical exposure.
Obturator Artery
Origin
- Branch of the anterior division of the internal iliac artery.
Course
- Arises within the pelvis.
- Passes through the obturator canal.
Branches
- Divides into:
- Anterior branch
- Posterior branch
These branches form a vascular circle around the obturator membrane.
Acetabular Branch
- A small branch of the obturator artery passes through the ligament of the head of the femur.
- It supplies a small portion of the femoral head.
Corona Mortis
Definition
- A vascular connection between:
- The obturator vessels (internal iliac system)
- The external iliac system, often through the inferior epigastric vessels.
Characteristics
- Often predominantly venous, although an arterial connection may also exist.
Location
- Typically located 3–7 centimeters from the pubic symphysis.
- Situated behind and superior to the superior pubic ramus.
Clinical Importance
- Can be injured during:
- Pelvic trauma
- Pelvic fracture surgery
- Ilioinguinal surgical approach
Complication
- Injury may result in significant hemorrhage that can be difficult to control.
Superior Gluteal Artery
Course
- Passes through the greater sciatic notch.
Clinical Significance
- May be injured in acetabular fractures involving the posterior column.
- Can also be damaged during posterior surgical approaches due to excessive retraction of the abductor muscles.
Medial Femoral Circumflex Artery
Importance
- The primary blood supply to the femoral head.
Potential Causes of Injury
- Traumatic hip dislocation.
- Surgical detachment of the quadratus femoris muscle from the femur instead of the ischium.
Surgical Consideration
- During surgical exposure, a small tendon attachment should be preserved to protect the deep branch of this artery.
Nerve Anatomy Related to the Acetabulum
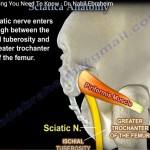
Sciatic Nerve
Relationship to the Acetabulum
- The sciatic nerve lies close to the posterior aspect of the acetabulum.
Incidence of Injury
- Sciatic nerve injury is the most common traumatic or iatrogenic nerve injury associated with acetabular fractures.
- Occurs in approximately 10 percent of hip dislocations.
- Risk increases in posterior acetabular fractures.
Clinical Examination
Assessment of sciatic nerve function should include:
- Testing ankle dorsiflexion
- Testing toe dorsiflexion
- Checking sensation over the dorsum of the foot
The peroneal division of the sciatic nerve is most commonly affected.
Important Practice
- Neurological examination should be repeated before surgery, as partial injuries may worsen after operative treatment.
Anatomical Relationship with Muscles
- The sciatic nerve lies:
- Posterior to the obturator internus muscle
- Inferior to the piriformis muscle
- Anatomical variations may occur, including splitting of the sciatic nerve around the piriformis muscle.
Surgical Precautions
- During posterior surgical approaches to the acetabulum:
- Keep the hip extended and knee flexed to reduce tension on the sciatic nerve.
- The obturator internus tendon can act as a protective layer between surgical retractors and the nerve.
Additional Nerves at Risk
Superior Gluteal Nerve
Location
- Close to the superior gluteal artery at the greater sciatic notch.
Risk of Injury
- May be injured during surgical approaches extending more than 5 centimeters above the greater trochanter.
- Excessive traction or attempts to control bleeding from the superior gluteal artery may damage the nerve.
Functional Consequence
- Injury may weaken the gluteus medius and gluteus minimus muscles.
- This results in hip abductor weakness and Trendelenburg gait.
Inferior Gluteal Nerve
Function
- Innervates the gluteus maximus muscle.
Possible Injury
- May be damaged during posterior hip approaches.
Lateral Femoral Cutaneous Nerve
Risk of Injury
- Can be injured during the ilioinguinal surgical approach.
Anatomical Course
- Usually passes beneath the inguinal ligament about 2 centimeters medial to the anterior superior iliac spine.
Clinical Effect
- Injury may cause sensory disturbances over the lateral thigh.
Summary Points
- The acetabulum is structurally divided into anterior and posterior columns.
- These columns form the inverted Y-shaped architecture of the pelvis.
- Important vessels related to the acetabulum include:
- Obturator artery
- Corona mortis
- Superior gluteal artery
- Medial femoral circumflex artery
- Important nerves at risk during trauma or surgery include:
- Sciatic nerve
- Superior gluteal nerve
- Inferior gluteal nerve
- Lateral femoral cutaneous nerve
Understanding this anatomy is essential for management of acetabular fractures and safe surgical approaches to the hip.
Leave a Reply