Courtesy: Ali Noorani, Shoulder Surgeon, London, UK
ACROMIOCLAVICULAR JOINT INJURIES
Objectives
- ACJ Joint Anatomy & Stability
- Classification of ACJ Instability
- Management of Acute Injuries
- Management of Chronic Injuries
- Techniques for fixation
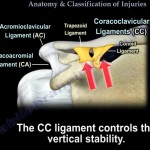
Stability
STATIC
- Every joint relies on Ligaments – acromioclavicular and coracoclavicular, bony Congruency and muscles around it in addition to a good functioning neurological system
- CC ligaments constitutes of conoid and trapezoid parts
DYNAMIC
– Deltotrapezial Fascia
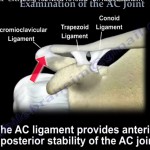
Anatomy
AC Joint Anatomy
– Diarthrodal Joint – Variety of Movements
– Intra-articular Disc (meniscus)
– Surrounded by capsule
– Thickest superiorly
– Thinnest inferiorly
Age & Diagnosis of Shoulder Pathologies
– 10 to 30 years
Instability ( Glenohumeral Joint & AC Joint )
Internal & Secondary Impingement
– 30 to 50 years
Primary Impingement Syndrome
Frozen Shoulder
AC Joint Pain
– 50 to 80 years
Full Thickness Cuff Tears
Arthritis
AC Separations
- Prevalence of Type 3 or higher- 14.5/100k per year
- Incidence depends on activity: 32% of professional Rugby players, 9% to 12% of traumatic shoulder injuries
- Associated intra-articular pathology> 15 %
Classification of AC Joint Separation
Type I
Sprain of the joint
Type II
- Some disruption of the AC ligaments
- Non-surgical injury’s only requiring rest and NSAIDs
Type III
- Superior dislocation of the AC joint with ruptured AC and CC ligaments
- TO FIX OR NOT TO FIX?
- Remains Controversial
Type IV
- Posterior displacement
Type V
- Highly Elevated
Type VI
- Inferior displacement
- All require surgical intervention
Treatment:
- 1 & 2 – These are stable and may be treated conservatively
- 3 Usually Non Operative initially. Consider Operative for Sports ( Throwers/Contact)
- 4/5 – these are unstable and require surgical management
- 6 Rare but Fix it
Surgical Considerations for type 3
Two different approaches
1.Fix Acutely
- Heavy Laborers
- High level athletes
- Patients not willing to accept cosmetic deformity
- Trade bump for Scar
2. Conservative approach
- Rest
- Ice
- Anti-inflammatories
- Continued pain or fatigue for > 3months = Surgery
- Usually done with addition of biologic graft
Classification
- Flawed. Not a linear deformity but 3D Rotational Deformity
- X-rays can show dynamic improvement
- 4/5 is probably the same
- Examination more important than the X-ray in decision making
- Low intra and inter observer reliability for the Rockwood classification
Acute or Chronic ACJ
- Acute 6 weeks
- Aim for Reconstruction
- Allograft, Autograft or Synthetic Ligament +/- Additional Stability
e.g Dog-Bone or Hook Plate
Surgical Treatment for Acute Injuries
- Address All Stabilisers of the Joint
- Periosteal sleeve avulsion of CC ligaments.
- Reduce Clavicle and hold it
- Stable e.g Dog Bone or Hook plate
- Repair Posterior Capsule of Joint
- Avoid resection of lateral end of clavicle. Remove IA Disc.
- Avoid further damage to Deltoid and Trapezius
- Mason-Allen repair of Deltotrapezial fascia
Surgical Treatment for Chronic Injuries
- Address All Stabilisers of the Joint
- Reconstruction of CC +/- AC ligaments & hold it stable e.g Dog Bone or Hook plate
- Repair Posterior Capsule of Joint
- Avoid resection of lateral end of clavicle. Remove IA Disc.
- Avoid further damage to Deltoid and Trapezius
- Mason-Allen repair of Deltotrapezial fascia
AC Joint Reconstruction
Important Considerations:
- Arthroscopic Technique (address associated pathology- 18% to 50% in reports)
- Open Technique Repairs the Deltotrapezial fascia and capsule
- Consider Combination
- Strength of construct
- Potential Complications
AC Joint Surgery
- Bosworth screw
- Weaver-Dunn
- Hook plate
- Tightrope
- Surgilig/Lockdown/Synthetic Ligament
- Auto or Allograft
- Arthrex Dog-Bone
ACCR Technique
- Anatomic Coracoclavicular Reconstruction
“Mazzocca” technique
Open technique for chronic AC reconstruction
Graft under coracoid using fibre wires and screws
Current Challenges in AC Joint Repair
- Hook Plate provides good stability but need removal.
- Risk of Acromion Injury and Cuff Injury
- Lockdown (Double braided Polyethyleneterephthalate (PET))
- Corocoid Fracture
- Musculocutaneous Nerve Injury
- Mal-Reduction or Residual Instability
- AC Internal Brace
Anterior/Posterior Stabilization with
- AC Internal Brace in conjunction with CC ligament fixation
Acromion:
- 3.5 mm BioComposite’M SwiveLocke
Distal Clavicle:
- 4.75 mm BioComposite SwiveLock
- FiberTape
Rehabilitation after ACJ Fixation
No Hand behind back, cross arm adduction, Any elevation >90, Extension and abduction
Remove Plate 3-5 Months
Key Points
- Shoulder Girdle / Scapula Injury
- Grade less important than assessment
- Rehab very Important
- Address Static and Dynamic Stabilizers
- Acute needs Stability
- Chronic needs Stability & Augmentation
Leave a Reply