Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Acromioclavicular (AC) Joint
Definition
The acromioclavicular (AC) joint is the articulation between:
-
The acromion of the scapula
-
The distal clavicle
It is a synovial plane joint that permits small gliding movements.
Stability of the AC Joint
AC joint stability is maintained by two major ligament groups:
-
Acromioclavicular (AC) ligament
-
Coracoclavicular (CC) ligaments
1. Acromioclavicular (AC) Ligament
Location
-
Extends between the acromion and clavicle
Function
-
Provides horizontal stability
-
Controls anterior–posterior translation of the clavicle
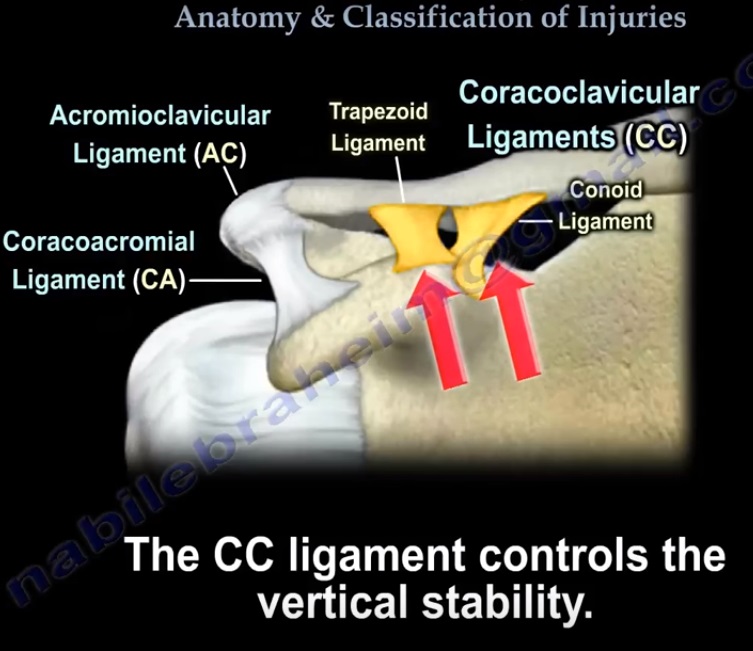
2. Coracoclavicular (CC) Ligaments
Role
-
Primary stabilizers of the distal clavicle
-
Prevent superior displacement of the clavicle
Components
-
Conoid ligament (medial)
-
Trapezoid ligament (lateral)
Conoid Ligament
Location
-
Medial component
Insertion
-
Approximately 4.5 cm from the distal clavicle
Function
-
Prevents superior displacement of the clavicle
Trapezoid Ligament
Location
-
Lateral component
Insertion
-
Approximately 3 cm from the distal clavicle
Function
-
Resists compression and axial forces
Coracoclavicular (CC) Distance
Definition
Distance between:
-
Coracoid process
-
Inferior surface of clavicle
Normal Value
-
< 12 mm
Clinical Significance
-
Increased distance suggests AC joint injury
Coracoacromial Ligament
Anatomy
-
Extends between:
-
Coracoid process
-
Acromion
-
Key Point
-
Does not contribute to AC joint stability
Surgical Importance
-
Can be used for reconstruction
(e.g., Weaver–Dunn procedure)
Mechanism of Injury
Common Cause
-
Direct trauma to the shoulder
Typical Scenario
-
Fall onto the point of the shoulder
Pathophysiology
-
Downward displacement of the acromion leads to ligament injury
Classification of AC Joint Injuries (Rockwood Classification)
AC joint injuries are classified into six types:
Type I Injury
Pathology
-
AC ligament sprain
-
CC ligaments intact
Clinical Features
-
Pain over AC joint
-
No displacement
Treatment
-
Nonoperative
Type II Injury
Pathology
-
AC ligament rupture
-
CC ligaments intact
Clinical Features
-
Partial displacement
-
Mild increase in CC distance
Treatment
-
Conservative
Type III Injury
Pathology
-
AC ligament rupture
-
CC ligament rupture
Clinical Features
-
Superior displacement of clavicle (up to 100%)
-
Increased CC distance
-
Deformity is reducible
Treatment
-
Controversial
-
Usually nonoperative
Surgical Consideration
-
Athletes
-
Heavy laborers
-
Persistent symptoms
Type IV Injury
Pathology
-
AC and CC ligaments ruptured
Clinical Features
-
Posterior displacement of clavicle
-
Clavicle displaced into trapezius muscle
Imaging
-
Best seen on axillary view X-ray
Treatment
-
Surgical
Type V Injury
Pathology
-
Severe ligament disruption
Clinical Features
-
100% superior displacement
-
Markedly increased CC distance
-
Severe deformity (not reducible)
Treatment
-
Surgical
Type VI Injury
Pathology
-
Rare injury
Clinical Features
-
Inferior displacement of clavicle
-
Clavicle lies below acromion or coracoid
-
Associated with high-energy trauma
Treatment
-
Surgical
Pediatric Considerations
Important Concept
In children, apparent AC dislocations are often:
-
Distal clavicle physeal injuries
Term
-
Pseudodislocation
Features
-
CC ligaments remain attached
-
Periosteal sleeve is intact
Treatment
-
Usually nonoperative
-
Excellent remodeling potential
Clinical Examination
Common Findings
-
Pain over AC joint
-
Prominent distal clavicle
-
Shoulder deformity
Reducibility Test
-
Reducible deformity ? Suggests low-grade injury
-
Irreducible deformity ? Suggests high-grade injury
Radiographic Evaluation
Standard Views
-
AP view
-
Axillary view
-
Zanca view
Zanca View
Technique
-
10° cephalic tilt
-
Reduced X-ray penetration
Advantage
-
Better visualization of the AC joint
Treatment Principles
Two main approaches:
-
Nonoperative treatment
-
Operative treatment
Nonoperative Treatment
Indications
-
Type I
-
Type II
-
Most Type III injuries
Management
-
Sling (approximately 1 week)
-
Early range of motion exercises
Possible Outcomes
-
Residual clavicle prominence
-
Occasional pain
-
Mild arthritis
Operative Treatment
Indications
-
Type IV, V, VI injuries
-
Selected Type III cases:
-
Athletes
-
Manual laborers
-
Chronic painful instability
-
Surgical Techniques
1. Coracoclavicular Ligament Reconstruction
Goal
-
Restore CC stability
Methods
-
Suture anchors
-
Button fixation
-
Sutures around coracoid
2. Hook Plate Fixation
Indication
-
Acute injuries
Limitations
-
Subacromial impingement
-
Hardware-related complications
3. Weaver–Dunn Procedure
Indication
-
Chronic AC dislocations
Steps
-
Distal clavicle excision
-
Transfer of coracoacromial ligament to clavicle
-
Often augmented with tendon graft
Chronic AC Dislocation (>4 Weeks)
Treatment
-
Tendon graft reconstruction
Common Grafts
-
Semitendinosus
-
Gracilis
Key Exam Points (Quick Revision)
Horizontal Stability
-
AC ligament
Vertical Stability
-
Coracoclavicular ligaments
CC Ligament Components
-
Conoid – medial
-
Trapezoid – lateral
Normal CC Distance
-
< 12 mm
Treatment Summary
Conservative
-
Type I
-
Type II
-
Most Type III
Surgical
-
Type IV
-
Type V
-
Type VI

Leave a Reply