Courtesy: Nirav Pandya MD, Associate Professor, Chief of Paediatric Orthopaedics, University of California at San Francisco(UCSF), USA
Pediatric Anterior Cruciate Ligament Injury
Introduction
- Previously considered rare in children
- Reason:
- Ligaments stronger than bone — injuries occurred at physis or tibial spine
- Reason:
Current Trend
- Rapidly increasing incidence
Why Increasing?
- Early sports specialization (age 6–10)
- High training load (20–30 hrs/week)
- Seen even in 7–9-year-olds
ACL Function
- Prevents:
- Anterior tibial translation (especially at ~30° flexion)
- Hyperextension
- Internal rotation
- Provides:
- Rotational + sagittal stability
Bundles
- Anteromedial bundle
- Posterolateral bundle
Current practice:
- Single bundle reconstruction
Unique Pediatric Considerations
Growth Plate (Physis)
- Major growth contributor:
- Distal femur
Surgical Risks
- Growth disturbance:
- Valgus deformity
- Recurvatum
- Limb length discrepancy (rare)
Natural History (Non-operative)
Earlier approach:
- Delay surgery
Problems with Non-operative Treatment
- Persistent instability
- Meniscus tears
- Early osteoarthritis (by early 20s)
Conclusion
- Non-operative treatment – poor outcomes
Failure Rates
- Pediatric ACL reconstruction:
- 10–25% failure
- Adults:
- 3–4%
High-Risk Group
- Age 12–14 years
- Most active
- Poor compliance
- Re-tear rate ~20%
Why Higher Failure in Children?
- High activity level
- Early return to sports
- Poor rehab compliance
Growth Disturbance Risk
- Overall risk:
- ~4%
Key insight:
- Preventing re-tear is more important than fear of physis injury
Clinical Features
History
- Acute:
- Pain + swelling
- Chronic:
- “Knee instability”
Acute Hemarthrosis Causes
Age 7–12
- ACL injury
- Meniscus tear
- Osteochondral fracture
- Patellar instability (commonest non-surgical)
Adolescents
- ACL injury > meniscus
Examination
- Difficult due to guarding
Key Tests
- Lachman test – Best to rule out
- Pivot shift – Best to confirm
- Anterior drawer – Less useful
Assessment of Skeletal Maturity
Do NOT rely only on age
Use
- X-ray (open/closed physis)
- Tanner staging
- Menarche (girls)
- Growth spurt history
- Height vs parents
Investigations
1. X-ray (First Step)
- Rule out:
- Tibial spine fracture
- Distal femur fracture
2. MRI
- Confirms:
- ACL tear
- Meniscus injury
- Cartilage damage
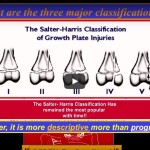
? Tibial Spine Fracture
Classification: Meyers & McKeever
- Type I – Conservative
- Type II – Trial reduction
- Type III – Surgery
Treatment Principles
Key Factors
- Skeletal maturity
- Activity level
- Compliance
- Growth remaining
Treatment Options
1. Non-operative
Not preferred
- Leads to instability + arthritis
2. Surgical Options
- Extra-articular
- Physeal-sparing
- Partial transphyseal
- Transphyseal
Graft Choice
Preferred
- Autograft
Options
- Hamstring
- Quadriceps tendon
- BTB (only skeletally mature)
Avoid
- Allograft
- 4× higher failure rate
Surgical Techniques (By Age)
| Stage | Technique |
|---|---|
| Tanner 1–2 | Physeal-sparing |
| Tanner 3–4 | Transphyseal |
| Tanner 5 | Adult reconstruction |
Technical Pearls
- Drill minimal physis (<7%)
- Use soft tissue graft
- Avoid bone plugs
Vertical tunnels:
- Protect physis
- BUT reduce rotational stability
Revision ACL
- Re-failure rate ~20%
- Poor outcomes
Golden Rule
- Avoid first failure
Risk Factors for ACL Injury
Modifiable
- Quadriceps dominance
- Weak core
- Poor neuromuscular control
- Dynamic valgus
Non-modifiable
- Female sex
- Narrow intercondylar notch
- Increased Q angle
Prevention
- Neuromuscular training programs
Example
- FIFA program:
- Reduces ACL injuries by ~75%
Exam Pearls (? High Yield)
- Pediatric ACL injuries – increasing incidence
- Non-operative – poor outcomes
- Early surgery – prevents arthritis
- Re-tear risk – 10–25%
- Most vulnerable – 12–14 years
- Growth disturbance – low (~4%)
- Autograft > allograft
- Prevention is critical

Leave a Reply