Courtesy: Saurabh Aggarwal, FRCS Orth, Princess ROyal University Hospital, London, UK
Vaughan Jackson Syndrome in the Rheumatoid Hand
Introduction
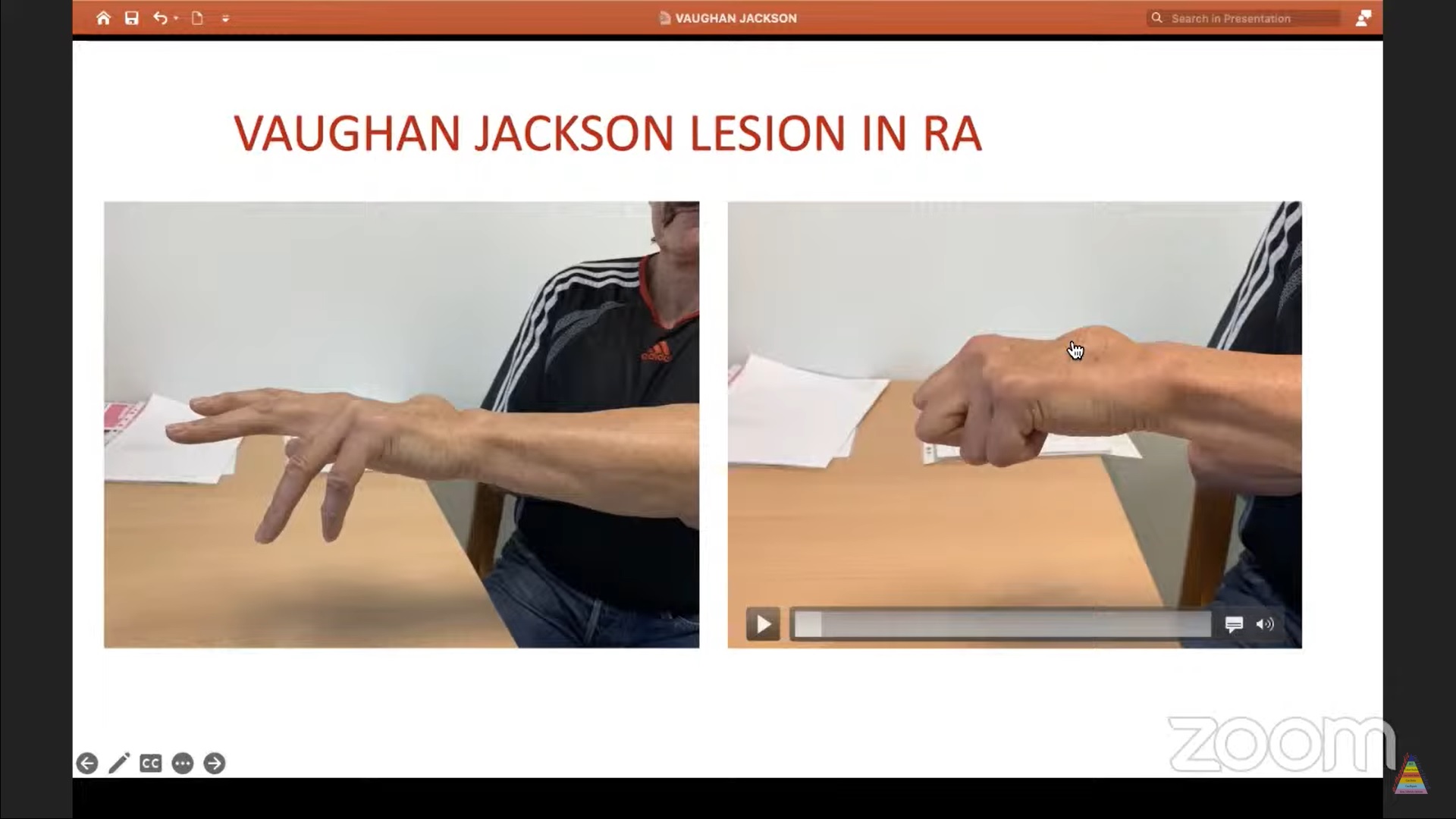
Vaughan Jackson syndrome refers to sequential extensor tendon ruptures in the rheumatoid hand caused by attritional wear over the distal ulna and distal radioulnar joint (DRUJ).
It is a classic complication of advanced rheumatoid arthritis involving:
- DRUJ synovitis
- Ulnar head instability
- Extensor tendon attrition
Rheumatoid Arthritis and Hand Pathology
Overview
Rheumatoid arthritis is a systemic autoimmune disorder characterized by chronic synovial inflammation.
Pathophysiology
Immune-mediated synovial inflammation leads to:
- Synovial proliferation
- Pannus formation
- Enzymatic destruction of soft tissues
Important enzymes involved include:
- Collagenases
- Proteases
- Elastases
Structures Affected
Progressive disease damages:
- Cartilage
- Ligaments
- Synovium
- Tendons
This eventually causes:
- Joint subluxation
- Joint destruction
- Deformity
- Tendon rupture
Causes of Dropped Fingers in Rheumatoid Arthritis
Several conditions may cause inability to extend the fingers.
Differential diagnoses include:
- Extensor tendon rupture (Vaughan Jackson syndrome)
- MCP joint synovitis
- Ulnar drift
- MCP volar subluxation
- Volar plate contracture
- Intrinsic muscle contracture
- Posterior interosseous nerve palsy
Clinical Differentiation
Ulnar Drift
Features include:
- Reduced active extension
- Passive correction possible
MCP Subluxation
Characteristics:
- Difficult passive correction
- Volar displacement at MCP joint
Contractures
Features:
- Loss of both active and passive extension
Tendon Rupture vs Nerve Palsy
Distinguished using the tenodesis effect.
Tenodesis Effect
Normal Response
- Wrist flexion causes finger extension
- Wrist extension causes finger flexion
Nerve Palsy
- Tenodesis remains intact
Tendon Rupture
- No finger movement during wrist motion
Loss of tenodesis suggests tendon rupture rather than nerve palsy.
Vaughan Jackson Syndrome
Cause
The syndrome results from:
- Dorsal subluxation of the ulnar head
- Mechanical attrition of extensor tendons
- Synovial pannus weakening the tendons
Sequence of Tendon Rupture
Tendon rupture typically progresses in a predictable order:
- Extensor Digiti Minimi (EDM)
- Extensor Digitorum Communis (EDC) to little finger
- EDC to ring finger
- Extensor Pollicis Longus (EPL)
- EDC to middle finger
- EDC and Extensor Indicis Proprius (EIP) to index finger
Ulnar Caput Syndrome
Pathology
Advanced DRUJ synovitis causes:
- Ligament destruction
- Cartilage erosion
- Dorsal subluxation of the ulnar head
The ECU tendon shifts volarly and is therefore usually spared.
The EDM tendon is commonly the first tendon to rupture.
Tendon Transfer Options
Single Tendon Rupture
Procedure
- EDM transferred end-to-side into ring finger EDC
Two Tendons Ruptured
Procedure
- EIP tendon transfer to reconstruct both tendons
Three Tendons Ruptured
Options include:
- EIP transfer to little and ring fingers using Pulvertaft weave
- End-to-side transfer from middle finger tendon to index tendon
- FDS tendon transfer
Four Tendons Ruptured
Procedure
- Two FDS tendons used
- Each tendon reconstructs two fingers
Management of Ulnar Head Pathology
Several procedures address DRUJ pathology.
Options include:
- Darrach procedure
- Sauvé-Kapandji procedure
- Hemiresection interposition arthroplasty (Bowers)
- Ulnar head prosthesis
An ulnar head prosthesis requires an intact sigmoid notch.
Clinical Case Example
Presentation
A 50-year-old male presented with:
- Inability to extend ring and little fingers
- Synovial swelling
- Advanced DRUJ arthritis
- Minimal MCP joint involvement
Diagnosis
Rheumatoid arthritis with:
- Mechanical tendon attrition
- Synovial pannus-related tendon degeneration
Intraoperative Findings
Findings included:
- Extensive synovitis
- Ruptured EDM tendon
- Ruptured EDC tendons to ring and little fingers
- Degenerated middle finger tendon
- Unhealthy index tendon
Surgical Reconstruction Strategy
Tendon Transfer Choice
EIP transfer was avoided because the index tendon was compromised.
Instead:
- Two FDS tendons were harvested
Technique
The FDS tendons were:
- Passed through the interosseous membrane
- Attached dorsally to reconstruct extensor function
Reconstruction
- One FDS tendon reconstructed little finger extension
- Another reconstructed ring and middle fingers
Additional Reconstruction
The extensor retinaculum was reinforced using:
- Palmaris longus graft
DRUJ Procedure
Management included:
- Ulnar head reshaping
- Capsular flap interposition
- Soft tissue arthroplasty using the Bowers technique
Postoperative Outcome
Outcome included:
- Mild extension lag of approximately 5–10°
- Functional hand restoration
- Good grip strength
- Improved usability
Rehabilitation Protocol
Early Motion
Early active motion is encouraged:
- Before day 5
- Or after day 10 depending on repair stability
Splinting
- Splinting for approximately 2–3 months
Exercises
- Active flexion exercises
- Passive extension exercises
Important Principle
Avoid prolonged immobilization because it increases:
- Adhesions
- Joint stiffness
Principles of Rheumatoid Hand Surgery
Management requires a multidisciplinary approach involving:
- Rheumatologists
- Hand therapists
- Hand surgeons
Goals of Surgery
- Pain relief
- Functional restoration
- Cosmetic improvement
Long-term follow-up and patient counseling are essential.
Important Clinical Sign
Horn Sign / Bunny Rabbit Sign
Test
The patient extends:
- Index finger
- Little finger
Significance
Indicates intact:
- EIP tendon
- EDM tendon
Useful when planning tendon transfer surgery.
 V
V

Leave a Reply