Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Ulnar Collateral Ligament (UCL) Injury of the Thumb MCP Joint
Introduction
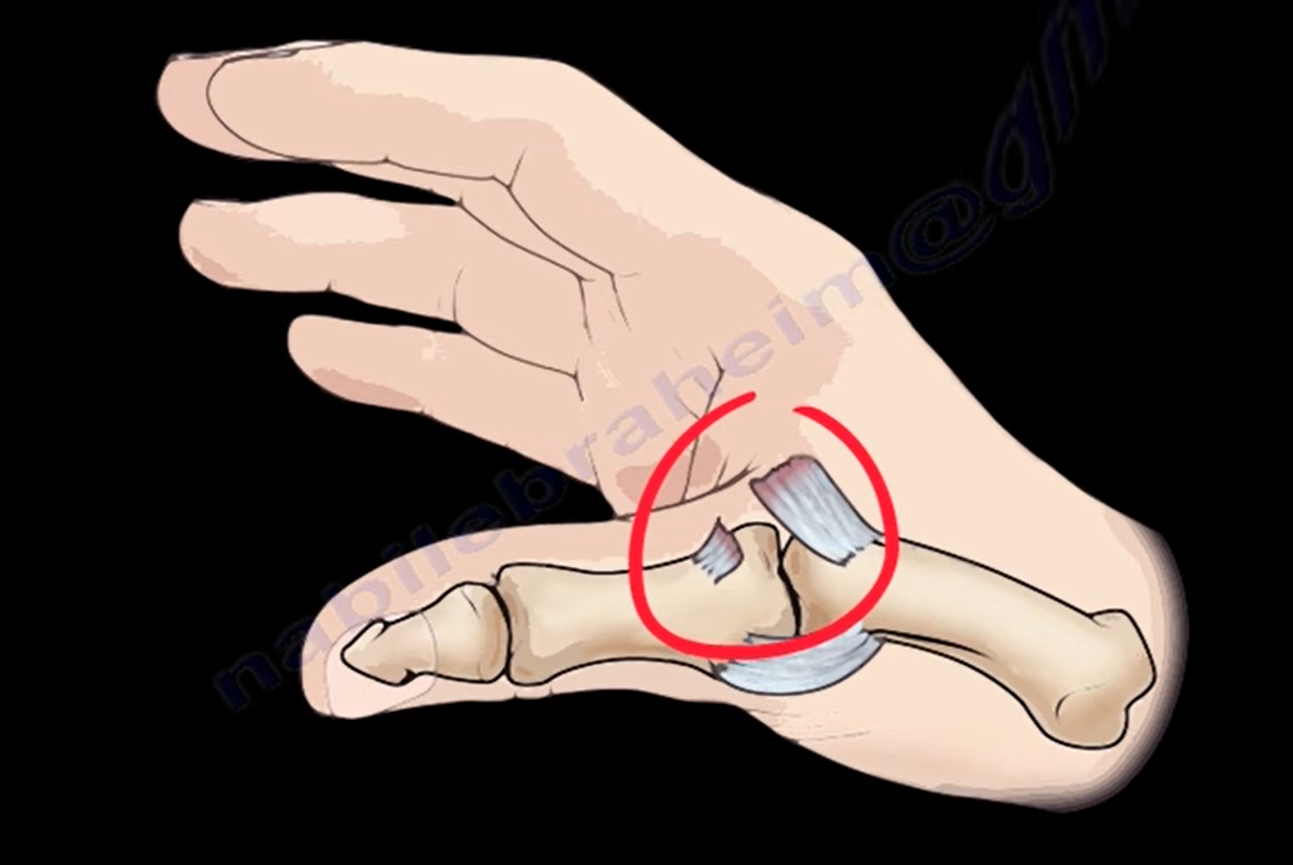
Injury to the ulnar collateral ligament (UCL) of the thumb metacarpophalangeal (MCP) joint is a common hand injury.
Clinical Importance
- Leads to MCP joint instability
- Impairs pinch and grip strength
Treatment aims to restore stability and function
Terminology
Skier’s Thumb
- Acute UCL injury
- Caused by sudden valgus force (e.g., skiing fall)
Gamekeeper’s Thumb
- Chronic UCL injury
- Due to repetitive stress
Mechanism of Injury
Typical Mechanism
- Valgus force on an abducted thumb MCP joint
Common Scenario
- Fall on an outstretched abducted thumb
Result
- Hyperabduction of MCP joint
- UCL tear
Epidemiology
Commonly Seen In
- Contact sports
- Non-contact sports
- Skiing injuries
- Young athletes
Site of Ligament Rupture
- ~80% occur at the distal insertion of UCL
- Located at base of proximal phalanx
Stener Lesion
Definition
Complete UCL tear with displacement superficial to the adductor aponeurosis
Mechanism
- Distal ligament retracts proximally
- Adductor aponeurosis interposes
Clinical Importance
Prevents spontaneous healing
Requires surgical repair
Incidence
- Present in ~80% of complete ruptures
Spectrum of Injury
- Mild sprain
- Partial tear
- Complete rupture
- Avulsion fracture
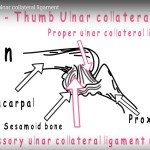
Anatomy of Thumb MCP UCL
Two Components
1. Proper UCL
- Origin: Dorsal metacarpal head
- Insertion: Volar base of proximal phalanx
Function
- Primary stabilizer in flexion
2. Accessory UCL
- Blends with:
- Volar plate
- Ulnar sesamoid
Function
- Stabilizer in extension
Functional Behavior
In Flexion
- Proper UCL — tight
- Provides valgus stability
In Extension
- Proper UCL — lax
- Accessory ligament + volar plate ? tight
Clinical Features
History
- Valgus injury
- Pain at ulnar MCP joint
- Difficulty in pinch
Symptoms
- Pain
- Swelling
- Ecchymosis
- Weak pinch
Examination Findings
- UCL tenderness
- Swelling
- Bruising
- Possible palpable mass (Stener lesion)
- Instability on stress testing
Valgus Stress Test
Important Rule
Always take X-ray before testing to rule out fracture
Testing Proper UCL
- MCP in 30° flexion
- Apply valgus stress
Positive Test
- 30° valgus laxity OR
-
15° compared to opposite thumb
Indicates proper UCL rupture
Testing Accessory UCL
- MCP in full extension
Interpretation
- <30° laxity – intact
- ?30° or >15° difference – complete rupture
Clinical Implication
- Instability in both flexion and extension
Both ligaments torn
High suspicion of Stener lesion
Imaging
X-ray
- Detects avulsion fractures
- May include stress views
MRI
- Confirms:
- Ligament tear
- Stener lesion
Consequences of Untreated Injury
- Chronic instability
- Weak pinch and grip
- Pain
- MCP joint arthritis
Treatment
Non-Operative Treatment
Indications
- Partial tear
- Stable joint
Method
- Thumb spica splint or cast
Duration
- 4–6 weeks
Rehabilitation
- Range of motion exercises
- Strengthening
Operative Treatment
Indications
- Complete rupture
- Valgus laxity –30°
-
15° difference from opposite side
- Stener lesion
- Instability in extension
Surgical Principles
- Anatomical ligament repair
- Restore alignment
- Remove interposed tissue (Stener lesion)
Chronic UCL Injury
Features
- Ligament attenuation
- Persistent instability
Treatment
- Ligament reconstruction
- Often using tendon graft
Prognosis
Early Treatment (<3 weeks)
- ~90% good to excellent outcomes
- Near-normal thumb function
Return to Sports
- High success rate
- Most athletes return to pre-injury level
Complications
- Persistent instability
- Weak pinch strength
- Chronic pain
- MCP arthritis
- Failure of repair
Key Take-Home Points
- Skier’s thumb — acute UCL injury
- Gamekeeper’s thumb — chronic injury
- Stener lesion requires surgery
- Flexion test — proper UCL
- Extension test — accessory UCL
- Early diagnosis leads to excellent outcomes
Leave a Reply