Courtesy: Mahdi Siala MD, Nice, France
Trapeziometacarpal (TMC) Dual Mobility Arthroplasty
Introduction
Trapeziometacarpal (TMC) arthroplasty has evolved significantly with the development of dual mobility prosthetic systems for thumb carpometacarpal (CMC) arthritis.
This approach aims to improve:
- Stability
- Range of motion
- Recovery time
- Functional outcomes
Modern dual mobility implants are inspired by hip arthroplasty concepts and are increasingly used in the treatment of thumb CMC osteoarthritis.
Functional Importance of the Thumb
The thumb is essential for:
- Fine pinch
- Precision grip
- Power grip
The thumb CMC joint must provide both:
- High mobility
- High stability
This creates a unique biomechanical challenge.
Biomechanics of the First CMC Joint
Joint Characteristics
Although traditionally described as a saddle joint, the first CMC joint behaves functionally like a complex ball-and-socket articulation.
Movements
The joint allows:
- Flexion and extension
- Abduction and adduction
- Axial rotation
- Pronation and supination
Joint Forces
The TMC joint experiences very high loads during pinch activities.
- Joint load may reach approximately 12 times the tip pinch force
- Forces may approach 1200 N during strong pinch
Stability of the TMC Joint
Because bony congruence is limited, stability depends mainly on:
- Ligaments
- Joint capsule
- Muscles
Important stabilizers include:
- Anterior oblique ligament (AOL)
- Dorsoradial ligament (DRL)
Ligament laxity is associated with development of CMC osteoarthritis.
CMC Osteoarthritis
Common Classification Systems
- Eaton-Littler classification
- Dell classification
Clinical Features
Patients commonly present with:
- Thumb base pain
- Reduced grip strength
- Weak pinch
- Loss of opposition
- Reduced abduction
- Loss of rotational movement
Goals of Surgical Treatment
An ideal procedure should:
- Preserve thumb length
- Maintain strength
- Preserve mobility
- Maintain fine motor and gross motor function
- Provide stability without stiffness
No single surgical procedure perfectly fulfills all these goals.
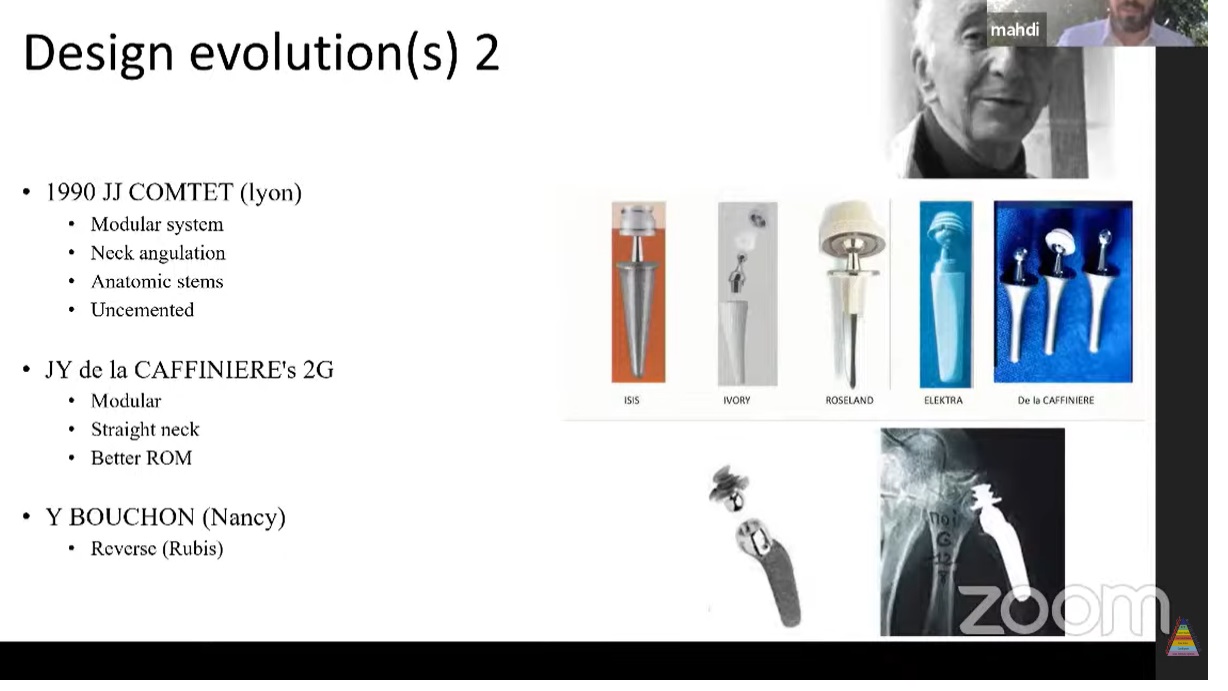
Historical Evolution of Surgical Treatment
Traditional Procedures
Historically used procedures include:
- Trapeziectomy
- Ligament reconstruction and tendon interposition (LRTI)
- Arthrodesis
Early Implant Arthroplasty
Early prosthetic designs introduced in the 1970s had high complication rates, including:
- Dislocation
- Implant loosening
- Mechanical failure
Modern Developments
Advances include:
- Modular implants
- Improved biomaterials
- Metal-polyethylene articulation
- Dual mobility systems
Dual Mobility Concept
The dual mobility concept originated from hip arthroplasty.
It was adapted for thumb CMC arthroplasty around 2010.
Advantages of Dual Mobility
Potential benefits include:
- Reduced dislocation risk
- Improved stability
- Better range of motion
- Improved function
Advantages of TMC Dual Mobility Arthroplasty
Reported benefits include:
- Restoration of thumb length
- Correction of Z-deformity
- Faster recovery compared with trapeziectomy
- Improved key pinch strength
- Low early revision rates
- Multiple revision options if failure occurs
Some studies report key pinch strength exceeding the opposite side after recovery.
Disadvantages
Limitations include:
- Technically demanding procedure
- Steep learning curve
- Higher implant cost
- Limited long-term outcome data
Surgical Principles
Surgical Approach
The dorsal approach is most commonly used.
Important structure to protect:
- Superficial radial nerve
Metacarpal Preparation
Proper exposure is essential.
Oversizing should be avoided because it may cause:
- Stress shielding
- Fracture risk
- Poor implant seating
Trapezium Preparation
This is considered the most critical step.
Important goals include:
- Preserving at least 6–8 mm of bone stock
- Proper cup positioning
- Stable fixation
Implant Positioning
The prosthetic cup should be:
- Centered
- Parallel to the articular surface
Fluoroscopy and trial reduction are recommended intraoperatively.
WALANT Technique
WALANT
Wide Awake Local Anesthesia No Tourniquet (WALANT) is increasingly used in hand surgery.
Advantages
Benefits include:
- No tourniquet discomfort
- Active intraoperative movement testing
- Immediate assessment of function
- Reduced cost
Clinical Outcomes
Reported short-term results include:
- Approximately 94% return to work within 6 weeks
- Implant survival rates around 96–97%
- Patient satisfaction rates of approximately 90–95%
Complications
Common Complications
- De Quervain’s tenosynovitis
- Superficial radial nerve irritation
- Trigger thumb
Less Common Complications
- Cup loosening
- Trapezium fracture
- Infection
Revision Surgery Options
Revision options include:
- Larger revision implant
- Alternative implant system
- Conversion to trapeziectomy
- Suspension arthroplasty
- Scaphometacarpal salvage procedures
Scaphotrapeziotrapezoid (STT) Arthritis
STT arthritis commonly coexists with thumb CMC arthritis.
In many patients:
- Treating the CMC joint alone adequately relieves symptoms
Separate treatment for STT arthritis is often unnecessary.
Patient Selection
Indications
- Symptomatic Stage II–IV CMC osteoarthritis
- Failure of conservative treatment
Contraindications
- Severe trapezium bone loss
- Poor bone quality
Special Situations
Heavy Manual Workers
Traditionally treated with arthrodesis, but arthroplasty is increasingly considered.
Inflammatory Arthritis
Can be treated successfully if deformity is manageable.
Implant Trends
Common dual mobility systems include:
- Touch
- Maya
- Moovis
There is an increasing trend toward dual mobility implants in thumb arthroplasty.
Material Considerations
Metal allergy, particularly nickel sensitivity, is uncommon but clinically relevant.
Some modern implants are now nickel-free.
Current Limitations and Evidence Gaps
Important limitations include:
- Lack of long-term follow-up data
- Variability in surgical technique
- Differences in implant systems
- Limited comparative trials
More standardized long-term studies are needed.
Conclusion
Dual mobility TMC arthroplasty represents a major advancement in the treatment of thumb CMC arthritis.
Potential advantages include:
- Better function
- Improved stability
- Faster recovery
- Lower early complication rates
However, limitations remain, including:
- Technical difficulty
- Learning curve
- Need for long-term evidence
Dual mobility arthroplasty may increasingly become a first-line surgical option for selected patients with thumb CMC osteoarthritis

Leave a Reply