Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Sacroiliac (SI) Joint Dysfunction
Introduction
Sacroiliac joint dysfunction is an important and frequently overlooked cause of low back pain.
It is increasingly recognized as a major contributor to:
- Chronic low back pain
- Persistent pain after lumbar fusion
- Failed back syndrome
Because symptoms often mimic lumbar disc disease or hip pathology, SI joint dysfunction can be difficult to diagnose.
Importance of the SI Joint
Epidemiology
The SI joint accounts for:
- Approximately 22% of low back pain cases
- Approximately 40% of pain after lumbar fusion surgery
Clinical Significance
Many patients with persistent pain after spinal surgery may actually have undiagnosed SI joint pathology.
Recognition of SI joint dysfunction can significantly improve patient outcomes and satisfaction.
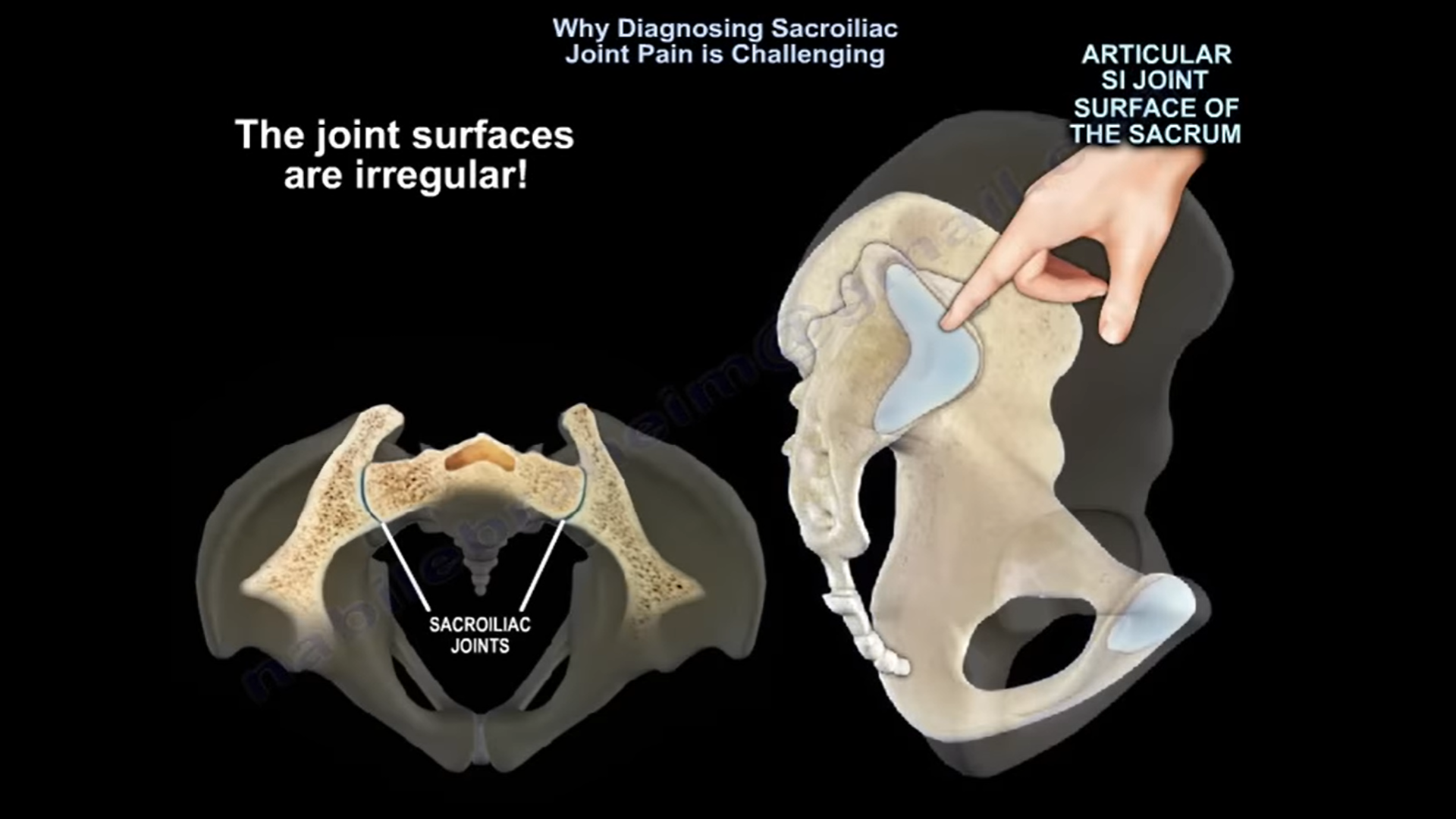
Anatomy and Function
Basic Anatomy
The sacroiliac joint connects:
- Sacrum
- Ilium of the pelvis
It functions as the mechanical link between:
- Spine
- Lower extremities
Function of the SI Joint
The SI joint is responsible for:
- Load transfer from spine to pelvis and lower limbs
- Shock absorption
- Pelvic stability
Joint Motion
The SI joint normally has minimal motion:
- Less than 4° rotation
- Approximately 1.6 mm translation
Excessive motion becomes pathological and may generate pain.
Pathophysiology
Source of Pain
Pain is believed to arise primarily from:
- Ligamentous structures surrounding the SI joint
These structures contain rich sensory innervation.
Important Concept
Pain is often related more to:
- Ligament strain
- Neural sensitization
- Neuroplasticity
rather than joint movement itself.
Risk Factors
Important risk factors include:
- Previous lumbar fusion surgery
- Multi-level spinal fusion
- Pregnancy and postpartum changes
- Pelvic trauma
- Twisting injuries
- Iliac crest bone graft harvesting
Inflammatory Conditions
Associated inflammatory disorders include:
- Ankylosing spondylitis
- Psoriasis
- Reactive arthritis
Biomechanical Factors
Additional contributors include:
- Scoliosis
- Leg length discrepancy
- Altered gait mechanics
Clinical Features
Pain Location
Typical pain characteristics include:
- Pain below L5
- Lateral rather than midline pain
- Pain around the posterior superior iliac spine (PSIS)
Radiation Pattern
Pain may radiate to:
- Buttock
- Posterior thigh
- Occasionally below the knee
This overlap may mimic sciatica.
Common Mimics
SI joint dysfunction can resemble:
- Lumbar disc herniation
- Radiculopathy
- Hip pathology
Aggravating Factors
Pain commonly worsens with:
- Sitting, especially on the affected side
- Climbing stairs
- Transitional movements
- Turning in bed
Relieving Factors
Symptoms often improve when the joint is unloaded.
Fortin Finger Test
Clinical Significance
This is a highly useful clinical sign.
Positive Test
The patient points within approximately 1 cm of the PSIS as the primary pain location.
This strongly suggests SI joint pathology.
Physical Examination
Provocative Tests
Diagnosis is supported when at least three provocative tests are positive.
Important Provocative Tests
Commonly used tests include:
- Compression test
- Thigh thrust test
- FABER test
- Distraction test
- Gaenslen’s test
Most Useful Test
The thigh thrust test is often considered the most sensitive provocative maneuver.
Additional Examination
Important associated findings:
- Straight leg raise usually negative
- Neurological examination usually normal
- Hip examination should be performed to exclude hip pathology
Imaging
Important Principle
Imaging alone is not diagnostic.
Imaging Findings
X-ray, MRI, and CT may show:
- Normal findings
- Degenerative changes
However, degenerative changes are also common in asymptomatic individuals.
Clinical correlation is essential.
Gold Standard Diagnosis
Diagnostic Injection
Image-guided SI joint injection is considered the gold standard for diagnosis.
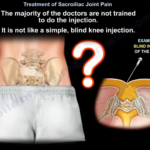
Technique
The procedure should include:
- Fluoroscopic or ultrasound guidance
- Low-volume anesthetic (<2 mL)
Diagnostic Criteria
Greater than 75% pain relief following injection strongly supports SI joint dysfunction.
Important Point
Blind injections are unreliable, with accuracy around 22%.
Treatment
Non-Operative Management
First-Line Treatment
Initial treatment includes:
- NSAIDs
- Physiotherapy
- Pelvic belt stabilization
Conservative therapy should generally continue for at least 4 weeks.
Injection Therapy
SI joint injections may serve both:
- Diagnostic
- Therapeutic purposes
Many patients experience symptom relief for several months.
Limitations
Repeated injections should generally be limited to:
- Maximum 3 injections within 6 months
Radiofrequency Ablation
Radiofrequency ablation targets posterior SI joint innervation.
However, results are variable because:
- The anterior SI joint cannot be fully denervated
Surgical Treatment
SI Joint Fusion
Indications
Surgery is considered for:
- Confirmed SI joint pain
- Failure of conservative treatment
Modern Surgical Approach
Current procedures are typically:
- Minimally invasive
- Outpatient-based
Outcomes
Properly selected patients often achieve:
- Better pain relief
- Improved function
- Better outcomes compared with prolonged conservative treatment
Impact on Quality of Life
SI joint dysfunction can severely affect daily functioning.
The disability burden may be comparable to:
- Hip arthritis
- Knee arthritis
and may exceed that seen in some chronic medical conditions such as COPD.
Key Clinical Pearls
- Pain below L5 with lateral localization strongly suggests SI joint pathology.
- Persistent pain after lumbar fusion should raise suspicion for SI joint dysfunction.
- SI joint pain commonly mimics lumbar radiculopathy and hip disease.
- Imaging alone is insufficient for diagnosis.
- Diagnostic injection remains the gold standard.
- At least three positive provocative tests improve diagnostic accuracy.
- Always evaluate both spine and hip pathology in patients with low back pain.

Leave a Reply