Courtesy: Dr Guri Ranum Ekas, Associate Professor, University of Oslo, Norway
General Overview
-
Discoid meniscus is a congenital anatomical variation of the meniscus.
-
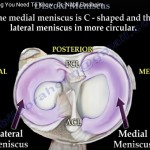
It most commonly involves the lateral meniscus of the knee.
-
The lateral meniscus normally exhibits greater mobility during knee flexion and extension.
-
Blood supply to the meniscus is limited and confined primarily to the peripheral zone.
CONGENITAL DISCOID MENISCUS
-
A developmental variation present from birth.
-
May account for up to 25 percent of meniscal surgeries in children.
-
More prone to:
-
Meniscal tears
-
Mechanical symptoms
-
Locking of the knee joint
-
WHAT IS A DISCOID MENISCUS?
-
Predominantly affects the lateral meniscus.
-
Frequently bilateral.
-
Characterized by:
-
Abnormal meniscal shape
-
Increased thickness
-
Possible instability due to abnormal attachments
-
INCIDENCE
-
True incidence remains unknown.
-
Estimated prevalence ranges from 3 to 15 percent.
-
Bilateral involvement is common.
MORPHOLOGY
-
Meniscus is:
-
Thicker than normal
-
Wider than normal
-
-
Covers a larger portion of the lateral tibial plateau.
MENISCAL INSTABILITY
-
Instability results from inadequate attachment to the joint capsule or tibia.
-
Instability may occur:
-
Anteriorly
-
Posteriorly (Wrisberg type)
-
In the midportion
-
STRUCTURAL CHARACTERISTICS
-
Reduced vascularity compared to a normal meniscus.
-
Fewer collagen fibers with disorganized orientation.
-
Increased susceptibility to rupture, especially horizontal tears.
-
Mucoid degeneration is frequently present.
CLASSIFICATION
Watanabe Classification (1969)
Based on arthroscopic assessment of morphology and stability:
-
Type 1: Stable, complete discoid meniscus
-
Type 2: Stable, incomplete discoid meniscus
-
Type 3: Unstable discoid meniscus (Wrisberg type)
-
Posterior attachment is only via the Wrisberg ligament
-
INCREASED RISK OF MENISCAL RUPTURE
-
Risk is increased up to 30 times compared to a normal meniscus.
-
Contributing factors include:
-
Increased thickness and width
-
Inferior meniscal tissue quality
-
Abnormal collagen orientation
-
Reduced vascularity
-
Mucoid degeneration
-
Mechanical instability
-
CLINICAL SYMPTOMS
-
Mechanical symptoms such as:
-
Popping
-
Snapping
-
Locking
-
-
Pain and swelling may be present.
-
Many patients remain asymptomatic unless rupture or instability occurs.
INSTABILITY AND DISLOCATION
-
An unstable discoid meniscus may dislocate intra-articularly during knee motion.
-
Displacement may occur:
-
Toward the intercondylar notch
-
Toward the peripheral compartment
-
-
May result in protrusion and joint locking.
AGE AT PRESENTATION
-
Children younger than 10 years:
-
Typically present with instability
-
Often bilateral
-
Usually not trauma related
-
-
Adolescents:
-
Symptoms often follow sports activities
-
-
Adults:
-
Symptoms typically follow minor trauma
-
CLINICAL EXAMINATION
-
May reveal:
-
Lateral joint line resistance
-
Palpable or audible clunk near full knee extension
-
Snapping knee phenomenon
-
RADIOGRAPHIC EVALUATION
Plain Radiography
-
Used as an initial investigation and for differential diagnosis.
-
Indirect signs may include:
-
Block-shaped lateral femoral condyle
-
Hypoplastic lateral tibial spine
-
Increased concavity of the lateral tibial plateau
-
Increased lateral joint space exceeding 11 millimeters
-
Magnetic Resonance Imaging
-
Confirms diagnosis.
-
Classic findings include the bow tie sign.
-
Allows assessment of associated meniscal tears and cartilage injury.
TREATMENT PRINCIPLES
-
No evidence supports prophylactic surgery in asymptomatic patients.
-
Initial rehabilitation is recommended for mild symptoms.
-
Surgical intervention is indicated for:
-
Persistent symptoms
-
Mechanical locking
-
-
A locked knee requires urgent surgical management.
SURGICAL MANAGEMENT OF SYMPTOMATIC DISCOID MENISCUS
Saucerization (Meniscal Sculpturing)
-
Removal of the central portion of the meniscus.
-
Preservation of a stable peripheral meniscal rim.
-
Repair of peripheral meniscal tears.
-
Central tears are generally not repairable.
-
Unstable meniscus should be stabilized.
INTRAOPERATIVE STEPS
-
Diagnostic arthroscopy to assess:
-
Meniscal width (complete or incomplete)
-
Meniscal height (normal or abnormal)
-
Peripheral stability
-
-
Saucerization to restore near-normal meniscal contour.
-
Suture repair of repairable peripheral tears.
-
Assessment and stabilization of peripheral attachments if instability is present.
SURGICAL CAUTION
-
Avoid excessive meniscal resection, especially in young children.
-
Preserve meniscal root attachments at all times.
POSTOPERATIVE MANAGEMENT
-
Saucerization without repair:
-
Weight bearing as tolerated
-
-
Saucerization with repair:
-
Partial weight bearing for 6 weeks
-
Use of crutches and optional orthosis
-
-
Structured physiotherapy program
-
Return to sports:
-
Individualized decision
-
Not earlier than 4 months postoperatively
-
PROGNOSIS
-
Total meniscectomy is associated with early onset osteoarthritis.
-
Saucerization with meniscal preservation provides:
-
Good clinical outcomes
-
Sustained results up to 10 years
-
SECONDARY COMPLICATIONS
-
Increased risk of articular cartilage damage.
-
Higher incidence of lateral femoral condyle osteochondritis dissecans.
Leave a Reply