Courtesy: Amr Abdelgawad, Maimonaides Medical centre, NY, USA
Overview
-
Regulation of blood clot formation and prevention is crucial in orthopaedic practice
-
Risk factors such as:
-
Surgery
-
Trauma
-
Prolonged immobilization
increase the likelihood of: -
Deep vein thrombosis (DVT)
-
Pulmonary embolism (PE)
-
A sound understanding of:
-
Coagulation cascade
-
Diagnosis of pulmonary embolism
-
Antithrombotic drugs
is essential for safe perioperative management
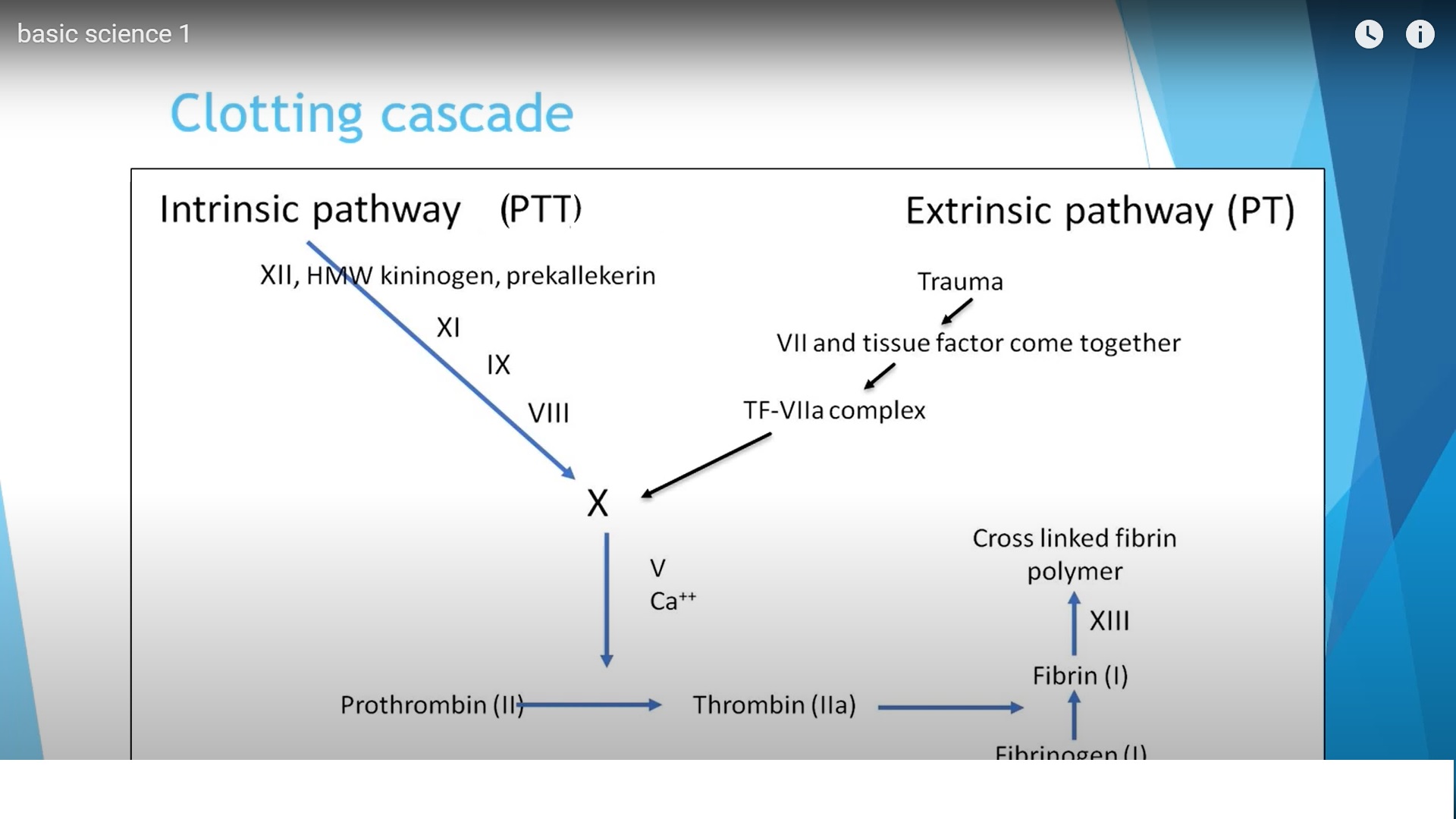
Coagulation Cascade
The coagulation cascade represents a series of enzymatic reactions leading to clot formation.
It consists of:
-
Extrinsic pathway
-
Intrinsic pathway
-
Common pathway
Extrinsic Pathway
Key Features
-
Activated rapidly after tissue injury
-
Initiated by tissue factor (TF) from outside the vessel
Mechanism
-
Tissue injury exposes factor VII to tissue factor
-
TF–factor VII complex activates factor X
Laboratory Assessment
-
Prothrombin Time (PT)
-
Standardized using INR (International Normalized Ratio)
Intrinsic Pathway
Key Features
-
Activated by circulating blood factors
-
Slower than extrinsic pathway
Factors Involved
-
Factor XII
-
Factor XI
-
Factor IX
-
Factor VIII
Outcome
-
Activation of factor X
Laboratory Assessment
-
Partial Thromboplastin Time (PTT)
Common Pathway
Convergence Point
-
Both pathways meet at factor X
Sequence
-
Factor X — Prothrombin — Thrombin
-
Thrombin — Fibrinogen — Fibrin
-
Factor XIII stabilizes fibrin
Result: Formation of a stable cross-linked fibrin clot
Pulmonary Embolism
Pulmonary embolism is a serious and potentially fatal complication, often arising from DVT, particularly in orthopaedic patients.
Clinical Presentation
-
Shortness of breath
-
Tachypnea
-
Chest pain
-
Tachycardia
-
Hypoxia (low oxygen saturation)
Initial Evaluation
-
Chest X-ray
-
ECG
-
Arterial blood gas (ABG)
Arterial Blood Gas Findings
Typical Findings
-
Hypoxemia
-
Hypocapnia (due to hyperventilation)
-
Respiratory alkalosis
-
Increased A–a oxygen gradient
Severe Cases
-
Hypercapnia
-
Respiratory acidosis
-
Metabolic acidosis (in shock)
ECG Findings
-
Sinus tachycardia
-
Possible right bundle branch block
Laboratory Markers
-
Elevated D-dimer
-
Increased natriuretic peptides (due to right ventricular strain)
Imaging in Pulmonary Embolism
CT Pulmonary Angiography (CTPA)
-
Gold standard in most settings
-
Direct visualization of thrombus in pulmonary arteries
-
Preferred in stable patients
Ventilation–Perfusion (V/Q) Scan
-
Assesses ventilation–perfusion mismatch
-
Less commonly used today
-
Useful when CTPA is contraindicated
Antithrombotic Medications
Unfractionated Heparin (UFH)
-
Large molecular compound
-
Enhances antithrombin activity
-
Inhibits:
-
Factor Xa
-
Thrombin (factor IIa)
-
Low Molecular Weight Heparin (LMWH)
-
Smaller molecules
-
Activates antithrombin
Key Feature
-
Greater inhibition of factor Xa than thrombin
Fondaparinux
-
Synthetic pentasaccharide
-
Selectively inhibits factor Xa via antithrombin
-
Does not inhibit thrombin
Direct Factor Xa Inhibitors
Examples
-
Rivaroxaban
-
Apixaban
Features
-
Direct inhibition of factor Xa
-
Oral administration
-
Do not require antithrombin
Direct Thrombin Inhibitors
-
Directly inhibit thrombin (factor IIa)
-
Available as:
-
Intravenous
-
Oral agents
-
Warfarin
-
Oral anticoagulant
Mechanism
-
Inhibits vitamin K epoxide reductase
-
Reduces activation of:
-
Factor II
-
Factor VII
-
Factor IX
-
Factor X
-
Pharmacology
-
Metabolized in the liver
-
Half-life: ~40 hours
Aspirin
-
Antiplatelet agent
Mechanism
-
Inhibits cyclooxygenase (COX)
-
Reduces thromboxane A2
-
Decreases platelet aggregation
Reversal and Drug Considerations
Warfarin
-
Metabolized in liver
-
Use cautiously in liver disease
Heparin & LMWH
-
Reversed by protamine sulfate
Fondaparinux & LMWH
-
Renal excretion
-
Avoid or use cautiously in renal failure
Dabigatran
-
Specific reversal agent available
Tranexamic Acid
Clinical Use
-
Widely used in orthopaedic procedures:
-
Joint replacement
-
Major fracture surgery
-
Benefits
-
Reduces perioperative blood loss
-
Supports clot stability
Mechanism of Action
-
Acts on the fibrinolytic pathway
-
Inhibits conversion of:
-
Plasminogen —} Plasmin
-
Effect
-
Reduces fibrin breakdown
-
Promotes stable clot formation
Key Takeaways
-
Orthopaedic patients are at high risk for DVT and PE
-
Coagulation cascade involves extrinsic, intrinsic, and common pathways
-
CTPA is the preferred imaging modality for PE
-
Anticoagulants act at different levels:
-
Factor Xa
-
Thrombin
-
Platelets
-
-
Drug selection depends on patient factors (renal function, bleeding risk)
-
Tranexamic acid plays a key role in reducing surgical blood loss
Leave a Reply