Courtesy: Amr Abdelgawad, Maimonaides Medical centre, NY, USA
Overview
– Blood clot formation and prevention are critical concepts in orthopedic surgery.
– Surgical procedures, prolonged immobilization, and trauma increase the risk of deep vein thrombosis and pulmonary embolism.
– Understanding the coagulation cascade, diagnostic features of pulmonary embolism, and mechanisms of antithrombotic medications is essential for safe perioperative management.
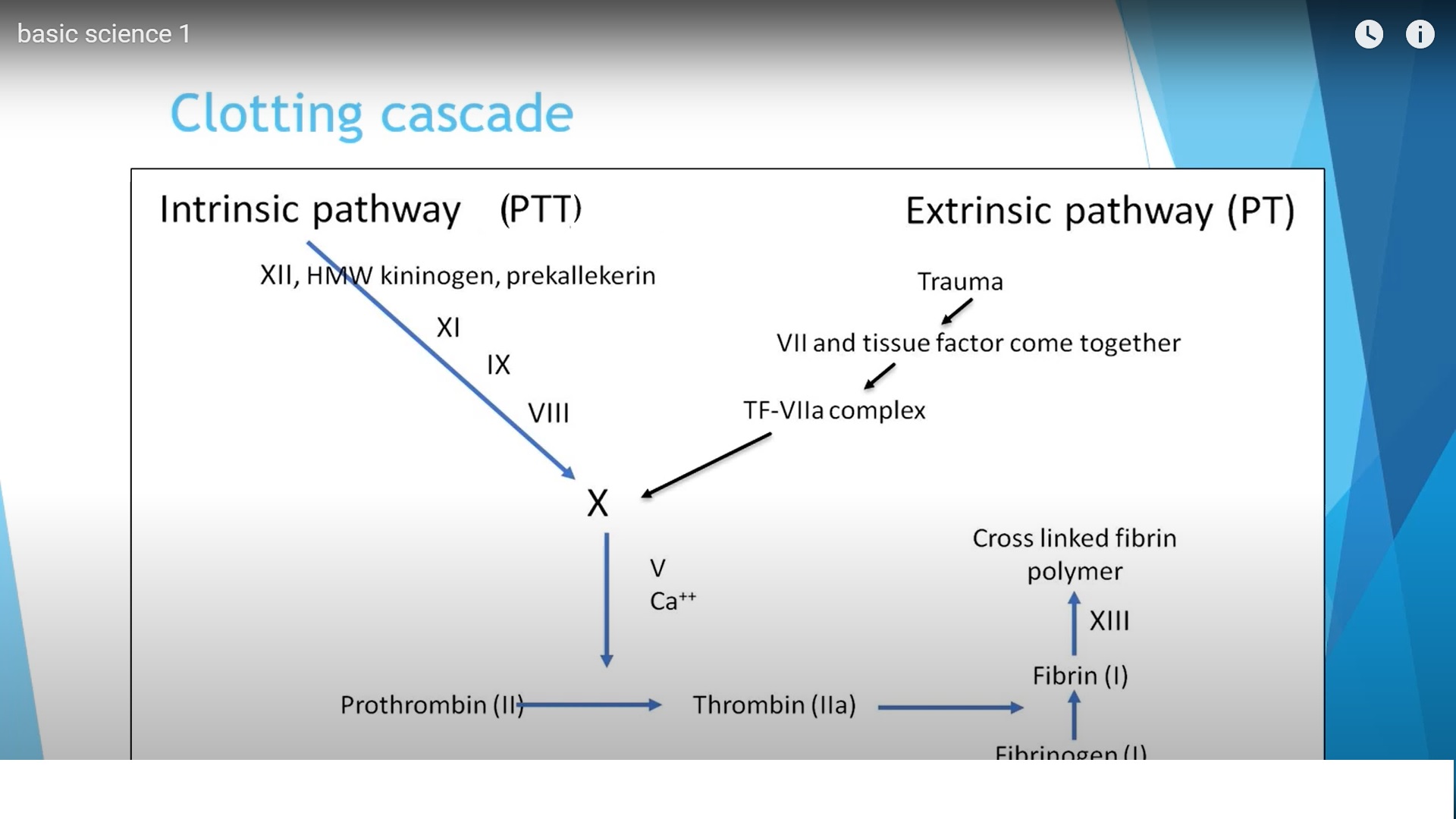
Coagulation Cascade
The coagulation cascade describes the sequence of biochemical reactions that lead to the formation of a blood clot. Two primary pathways initiate coagulation before merging into a common pathway.
Extrinsic Pathway
– The extrinsic pathway is activated rapidly after tissue injury.
– It involves tissue factor that originates outside the blood vessel.
– Trauma exposes circulating factor VII to tissue factor present in surrounding tissues.
– The tissue factor–factor VII complex activates factor X.
– Laboratory assessment is performed using the prothrombin time test.
– The international normalized ratio is used to standardize prothrombin time measurements.
Intrinsic Pathway
– The intrinsic pathway is activated by factors present within the blood circulation.
– This pathway involves factors XII, XI, IX, and VIII.
– These factors collectively activate factor X.
– Laboratory assessment is performed using the partial thromboplastin time test.
– The intrinsic pathway takes longer to activate compared with the extrinsic pathway.
Common Pathway
– Both intrinsic and extrinsic pathways converge at factor X.
– Activated factor X converts prothrombin into thrombin.
– Thrombin converts fibrinogen into fibrin.
– Fibrin molecules polymerize and are stabilized by factor XIII.
– Cross-linked fibrin forms the structural framework of the final blood clot.
Pulmonary Embolism
Pulmonary embolism is a major complication associated with deep vein thrombosis and orthopedic surgery. Large emboli can obstruct pulmonary circulation and may be life threatening.
Clinical Presentation
– Shortness of breath
– Increased respiratory rate
– Chest discomfort
– Rapid heart rate
– Reduced oxygen saturation
Initial Diagnostic Evaluation
– Chest radiography
– Electrocardiography
– Arterial blood gas analysis
Arterial Blood Gas Findings
– Reduced oxygen levels in the blood
– Reduced carbon dioxide levels due to hyperventilation
– Respiratory alkalosis caused by increased ventilation
– Increased alveolar–arterial oxygen gradient
Severe cases may show:
– Increased carbon dioxide levels
– Respiratory acidosis
– Metabolic acidosis in cases of shock
Electrocardiographic Findings
– Sinus tachycardia
– Possible right bundle branch block
Laboratory Findings
– Elevated D-dimer levels
– Increased natriuretic peptides due to right ventricular strain
Imaging Studies
Computed Tomography Pulmonary Angiography
– Commonly used diagnostic imaging modality
– Detects thrombi within pulmonary arteries
– Preferred when the patient is stable enough for imaging
Ventilation–Perfusion Scan
– Nuclear imaging technique assessing ventilation and perfusion
– Demonstrates ventilation–perfusion mismatch
– Used less frequently today
Antithrombotic Medications
Unfractionated Heparin
– Large molecular compound
– Enhances activity of antithrombin
– Inhibits activated factor X and thrombin
Low Molecular Weight Heparin
– Smaller molecules compared with unfractionated heparin
– Activates antithrombin
– Stronger inhibition of activated factor X than thrombin
Fondaparinux
– Synthetic pentasaccharide
– Activates antithrombin
– Selectively inhibits activated factor X
– Does not inhibit thrombin
Direct Factor X Inhibitors
– Directly inhibit activated factor X
– Examples include rivaroxaban and apixaban
– Administered orally
– Do not require antithrombin
Direct Thrombin Inhibitors
– Direct inhibition of thrombin
– Available as intravenous and oral agents
Warfarin
– Oral anticoagulant
– Inhibits vitamin K epoxide reductase
– Reduces activation of clotting factors II, VII, IX, and X
– Metabolized in the liver
– Average half-life approximately 40 hours
Aspirin
– Acts on platelets
– Inhibits cyclooxygenase enzyme
– Reduces thromboxane A2 production
– Decreases platelet aggregation
Reversal and Metabolism of Anticoagulants
Warfarin
– Metabolized in the liver
– Requires caution in liver disease
Heparin and Low Molecular Weight Heparin
– Anticoagulant effect reversed with protamine sulfate
Fondaparinux and Low Molecular Weight Heparin
– Eliminated through the kidneys
– Contraindicated or used with caution in renal failure
Dabigatran
– Oral direct thrombin inhibitor
– Specific reversal agent available
Tranexamic Acid
Clinical Role
– Used in orthopedic procedures including joint replacement and major fracture surgery
– Reduces perioperative blood loss
– Supports formation of stable blood clots
Mechanism of Action
– Targets the fibrinolytic pathway
– Prevents conversion of plasminogen into plasmin
– Reduces breakdown of fibrin clots
– Stabilizes formed blood clots
Leave a Reply