Courtesy: Pierre Laumonerie MD, Paris, France
Overview
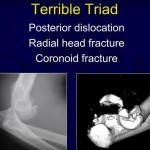
- Term “Terrible Triad of the Elbow” coined in 1996 by O’Driscoll.
- Involves posterior elbow dislocation, radial head fracture, and coronoid process fracture.
- Historically poor outcomes due to complex instability.
Anatomical Background
- Lateral Collateral Ligament (LCL) Complex:
- Includes radial collateral ligament and ulnar collateral ligament.
- Plays role in posterolateral stability, less in varus stability.
- Medial Collateral Ligament (MCL):
- Anterior and posterior bundles.
- Major contributor to valgus stability.
- Posterolateral Rotatory Instability (PLRI):
- Key instability pattern in terrible triad.
- First described by Regan & Morrey.
Mechanism of Injury
- Common mechanism: fall on outstretched hand with axial load, valgus stress, and supination.
- Radial head and coronoid fractures dissipate force, preventing complete dislocation in some cases.
Historical Understanding & Evolution
- O’Driscoll’s Circle of Hori:
- Injury progresses lateral to medial.
- Stages of instability based on sequential failure of soft tissue and bone.
- Newer model (Rüegsegger et al):
- “Reverse Circle of Horii”—injury may begin medially.
- Emphasizes MCL rupture and valgus force.
Surgical Principles
- Goal: Achieve elbow stability for early mobilization and function.
- Fixation of all components improves outcome:
- Radial head
- Coronoid process
- LCL complex
Radial Head Fracture
- Usually results from impaction under the capitellum.
- Fixation Techniques:
- Small central fragments removed.
- Disimpaction followed by screw or tripod fixation.
- Plates are used for comminuted or unstable neck fractures.
- Arthroplasty:
- Preferred when reconstruction is not feasible.
- Yields better results than overaggressive fixation attempts.
Coronoid Process Fracture
- Usually involves tip fracture (capsular attachment site).
- Term: “Capsular Fracture” reflects functional disruption.
- Treatment Options:
- Non-operative in minor cases with stable elbow after other repairs.
- Anchors or screws used if instability persists.
- Retrograde screw or plate fixation in transverse or more severe fractures.
LCL and MCL Repair
- LCL (Lateral Ulnar Collateral Ligament):
- Always repaired in terrible triad.
- MCL Repair:
- Indicated in:
- High functional demand (e.g. athletes)
- Persistent valgus or posterolateral instability
- Obese patients with gravitational varus stress
- When radial head and LCL repair insufficient
- Indicated in:
Fixation Strategy Based on Stability Goals
- Fixation priority is joint stability, not just bone anatomy.
- “Fix it, Move it” principle:
- More stable fixation allows earlier mobilization.
- Leads to improved outcomes and lower osteoarthritis risk.
Summary & Modern Perspective
- The historical “terrible” prognosis is outdated.
- Better understanding of biomechanics has revolutionized management.
- Early, systematic fixation of key stabilizers—radial head, coronoid, LCL, and when needed MCL—is key.
- Emphasis on individualized approach based on:
- Functional demand
- Obesity and soft tissue stresses
- Preoperative elbow stability


Leave a Reply