Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
ANATOMY
-
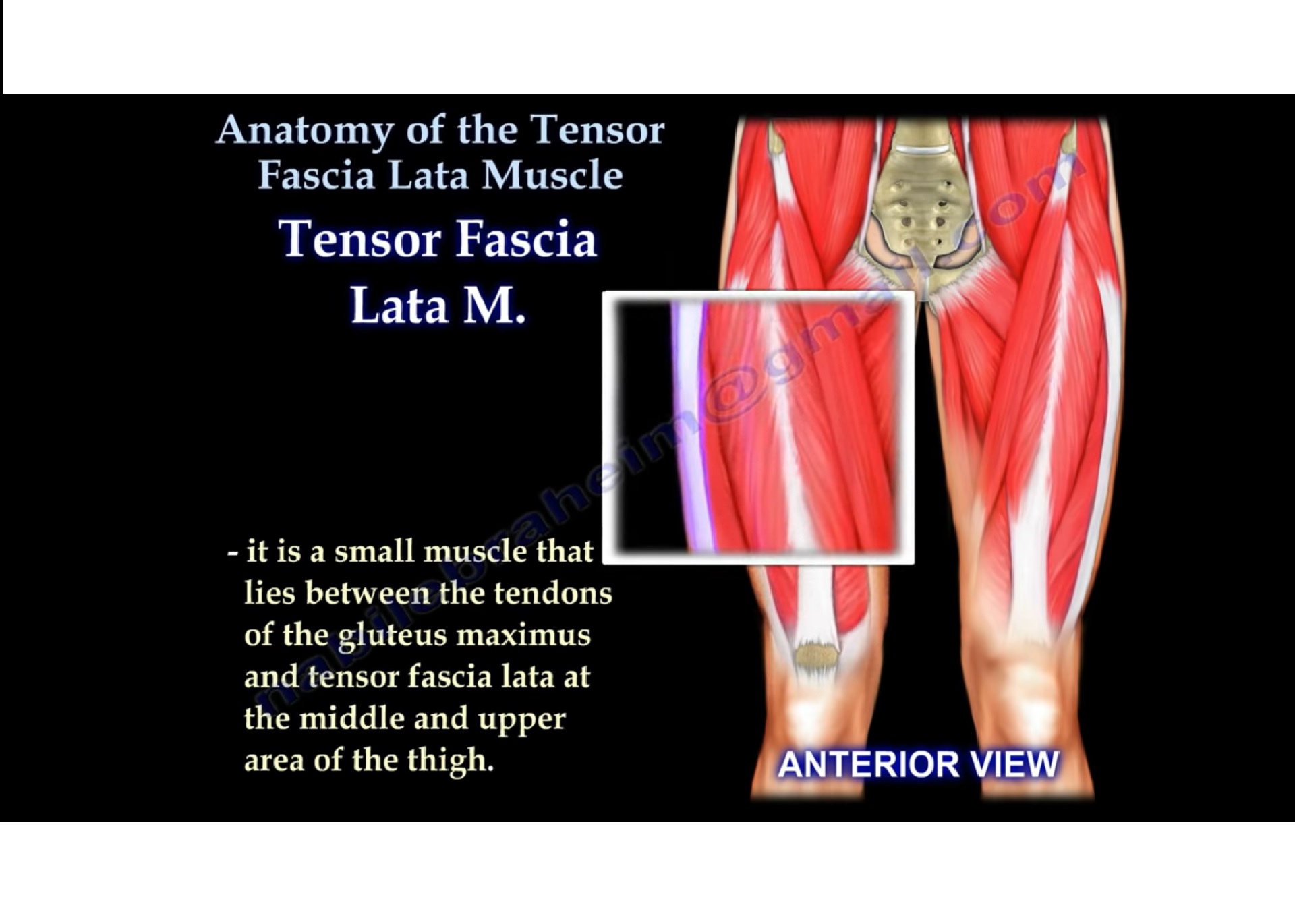
The tensor fascia lata is a small, flat muscle located in the anterolateral aspect of the upper thigh.
-
It lies between:
-
The gluteus maximus posteriorly
-
The fascia lata and iliotibial tract laterally
-
-
It blends distally with the iliotibial band, contributing to lateral thigh stability.
ORIGIN
-
Arises from the anterior part of the outer lip of the iliac crest.
-
Also takes origin from the anterior superior iliac spine.
INSERTION
-
Inserts into the iliotibial band.
-
The iliotibial band extends from the iliac crest to the lateral condyle of the tibia, where it attaches at Gerdy tubercle.
FASCIAL ANATOMY
-
The iliotibial band is a thickened lateral band of fascia.
-
It runs along the lateral thigh from the iliac crest to the knee.
-
It plays a key role in lateral knee and hip stability.
INNERVATION
-
Supplied by the superior gluteal nerve.
-
The nerve exits the pelvis through the greater sciatic foramen above the piriformis muscle.
FUNCTION
-
Assists in hip flexion.
-
Assists in hip abduction.
-
Contributes to internal rotation of the thigh.
-
Helps stabilize the pelvis during single-leg stance.
-
Counteracts the posterior pull of the gluteus maximus on the iliotibial band.
ASSOCIATED CLINICAL CONDITIONS
1. Snapping Hip Syndrome (External Type)
-
Caused by the iliotibial band sliding over the greater trochanter.
-
Produces an audible or palpable snapping sensation.
-
Often painful during hip motion.
Clinical Examination
-
Patient lies in the lateral position.
-
Hip is placed in extension and rotated.
-
Examiner slowly abducts the leg with the knee flexed.
-
Tight iliotibial band results in:
-
Limited abduction
-
Reproducible snapping sensation
-
2. Trochanteric Bursitis
-
Results from repetitive friction, trauma, or irritation of the iliotibial band over the greater trochanter.
-
Leads to inflammation of the trochanteric bursa.
-
Patients typically localize pain directly over the lateral aspect of the hip.
3. Iliotibial Band Syndrome (Runner’s Injury)
-
Commonly seen in long-distance runners.
-
Caused by repetitive friction between the iliotibial band and the lateral femoral condyle.
-
Presents with lateral knee pain during activity.
Treatment
-
Activity modification
-
Physical therapy
-
Local injection therapy
-
Surgical intervention in refractory cases
4. Thigh Compartment Syndrome
Surgical Approaches Involving Tensor Fascia Lata
Watson–Jones Approach
-
Interval between:
-
Tensor fascia lata
-
Gluteus medius
-
-
Both muscles are supplied by the superior gluteal nerve.
Smith–Petersen Approach
-
Interval between:
-
Tensor fascia lata (superior gluteal nerve)
-
Sartorius muscle (femoral nerve)
-
-
Care must be taken to protect the lateral femoral cutaneous nerve of the thigh.
CLINICAL RELEVANCE
-
The tensor fascia lata plays a critical role in hip biomechanics and lateral thigh stability.
-
Dysfunction can contribute to:
-
Hip pain
-
Knee pain
-
Gait abnormalities
-
-
It is an important landmark in orthopaedic surgical approaches to the hip and thigh.
Its really nice and informative
thank you so much