Courtesy: Prof Nabil Ebraheim
Tennis Elbow (Lateral Epicondylitis)
Overview
Tennis Elbow, also known as lateral epicondylitis, is one of the most common causes of lateral elbow pain.
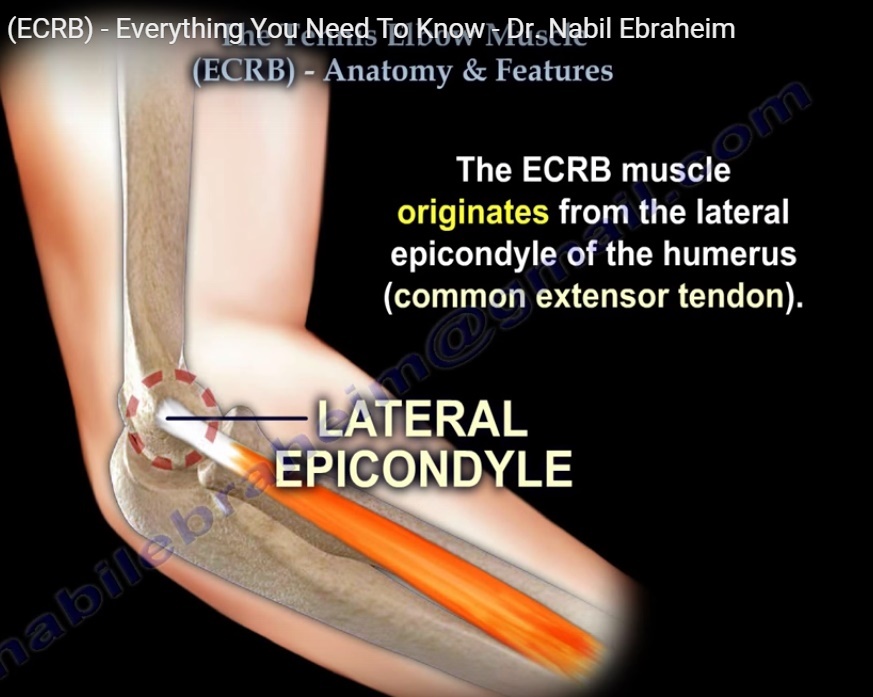
It is an overuse injury involving degeneration and tendinosis of the origin of the extensor carpi radialis brevis (ECRB) tendon at the lateral epicondyle of the humerus.
Anatomy and Pathophysiology
Primary Muscle Involved
The main muscle involved is the:
- Extensor Carpi Radialis Brevis (ECRB)
Origin
- Lateral epicondyle of the humerus
- Common extensor tendon
Insertion
- Base of the third metacarpal
Function
- Wrist extension
- Radial deviation (abduction) of the wrist
Innervation
- Radial nerve
The ECRB tendon is particularly vulnerable to repetitive eccentric overload.
Pathology
Histological Findings
Despite the term “epicondylitis,” the condition is primarily degenerative rather than inflammatory.
Common findings include:
- Disorganized collagen
- Angiofibroblastic hyperplasia
- Fibroblast hypertrophy
- Microtears at the tendon origin
- Vascular granulation tissue
This process is better described as tendinosis.
Causes and Risk Factors
Sports-Related Causes
Approximately 40–50% of tennis players may develop symptoms due to:
- Poor swing mechanics
- Incorrect grip size
- Repetitive backhand strokes
- Excessive wrist extension
Occupational Causes
Common in individuals performing:
- Repetitive gripping
- Heavy lifting
- Tool use
- Manual labor
Repetitive wrist extension and forearm pronation increase stress on the ECRB tendon.
Clinical Presentation
Symptoms
Patients commonly complain of:
- Lateral elbow pain
- Pain during gripping
- Weak grip strength
- Pain with lifting objects
- Pain during repetitive wrist extension
- Difficulty with daily activities such as carrying groceries
Pain may also interfere with sleep.
Physical Examination
Tenderness
Point tenderness is typically located over:
- The lateral epicondyle
- ECRB origin
Provocative Test
Pain increases with:
- Resisted wrist extension
- Elbow fully extended
This is a classic examination finding.
Differential Diagnosis
Radial Tunnel Syndrome
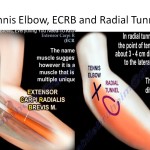
Radial Tunnel Syndrome should always be considered, especially if symptoms fail to improve as expected.
Key Differences
| Tennis Elbow | Radial Tunnel Syndrome |
|---|---|
| Tenderness directly over lateral epicondyle | Tenderness 3–5 cm distal and anterior to lateral epicondyle |
| Tendinopathy | Nerve compression |
| Pain with resisted wrist extension | Deep aching forearm pain |
Radial tunnel syndrome involves compression of the posterior interosseous nerve.
Other Differential Diagnoses
Additional conditions to exclude include:
- Cervical radiculopathy
- Posterior interosseous nerve syndrome
- Triceps tendinopathy
- Osteoarthritis of the elbow
Imaging
X-rays
Usually normal.
Occasionally may show:
- Calcification near the extensor origin
Imaging is mainly used to exclude other pathology.
Nonoperative Treatment
First-Line Management
Most patients improve without surgery.
Treatment Options
- Activity modification
- NSAIDs
- Ice therapy
- Physiotherapy
- Bracing or counterforce straps
Physiotherapy
Particularly effective interventions include:
- Eccentric strengthening exercises
- Tendon gliding exercises
- Stretching programs
Evidence suggests physiotherapy provides better long-term relief than corticosteroid injections.
Injection Therapy
Corticosteroid Injection
May provide short-term symptom relief.
Important Considerations
- Useful for acute pain control
- Repeated injections should be limited
- Excessive steroid use may weaken tendon tissue
PRP Injection
Platelet-rich plasma (PRP) may be used in chronic cases, although evidence remains variable.
Ultrasound guidance can improve injection accuracy.
Prognosis
Success Rate
Approximately:
- 90–95% improve with conservative treatment
Recovery may take:
- 6–12 months
Most cases eventually resolve regardless of the specific conservative method used.
Surgical Treatment
Indications
Reserved for patients with:
- Persistent symptoms
- Failed prolonged nonoperative treatment
Procedure
Typical surgery involves:
- Debridement of diseased ECRB tendon
- Release of the ECRB origin
Surgical Complication
Posterolateral Rotatory Instability (PLRI)
Excessive release near the lateral collateral ligament complex can injure the:
- Lateral ulnar collateral ligament (LUCL)
This may result in:
Posterolateral Rotatory Instability
Important Associated Conditions
Intersection Syndrome
Definition
An overuse inflammatory condition occurring where:
- First dorsal compartment tendons cross
- Second dorsal compartment tendons
The second compartment contains:
- ECRB
- Extensor carpi radialis longus (ECRL)
Clinical Findings
Pain is usually:
- Dorsoradial forearm
- Approximately 4–6 cm proximal to the wrist
Common in repetitive wrist extension activities.
ECRB in Surgical Approaches
Thompson Dorsal Approach
The interval between:
- ECRB
- Extensor digitorum
is used to expose the proximal radius.
Tendon Transfer in High Radial Nerve Palsy
Important Transfer
In Radial Nerve Palsy:
- Pronator teres may be transferred to ECRB
Purpose
To restore:
- Wrist extension
- Functional hand positioning
Related Posts
 Tennis Elbow
Tennis ElbowCourtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA …
 Tennis Elbow Revisited
Tennis Elbow RevisitedCourtesy: Christian Schoch, Shoulder and Elbow Surgeon, Pfronten, Germany
 Tennis Elbow and ECRB
Tennis Elbow and ECRBCourtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Leave a Reply