Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
TARSAL TUNNEL SYNDROME
- Compressive neuropathy of the posterior tibial nerve or its branches within the tarsal tunnel
- Tarsal Tunnel- a fibro-osseous space located on the medial side of the ankle
- Equivalent to carpal tunnel syndrome
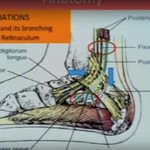
ANATOMY OF TARSAL TUNNEL
- Narrow fibro-osseous passage located on the medial side of the ankle, just posterior and inferior to the medial malleolus.
- Serves as a conduit for several important neurovascular and tendinous structures that pass from the leg into the foot.
BOUNDARIES
- Roof: Flexor retinaculum (laciniate ligament), a strong fibrous band that stretches from the medial malleolus to the calcaneus.
- Floor: Medial surfaces of the talus, calcaneus, and the distal tibia.
CONTENTS
- Tibialis posterior tendon
- Flexor digitorum longus tendon
- Posterior tibial artery
- Posterior tibial vein(s)
- Tibial nerve
- Flexor hallucis longus
TIBIAL NERVE
- Origin :- One of the two terminal branches of the sciatic nerve(tibial nerve and common peroneal nerve)
- Motor and sensory innervation to the posterior leg and plantar surface of the foot.
- Root value:- L4–S3.
COURSE
- Arises from the apex of popliteal fossa
- Descends vertically through the popliteal fossa lying superficial to the popliteal artery and vein.
- Passes deep to the tendinous arch of soleus and runs between the superficial and deep flexor muscles
- Travels down the posterior compartment of the leg, accompanying the posterior tibial vessels
- In the ankle it passes behind the medial malleolus that is through the tarsal tunnel and terminate as medial and lateral plantar nerves.
BRANCHES
IN THE POPILITEAL FOSSA
Muscular branches:-
- Gastrocnemius (Medial and lateral head)
- Soleus
- Plantaris
- Popliteus
- Cutaneous branches
- Sural nerve:-Provides sensation to the posterior leg and lateral foot
- Articular branches to the knee joint
IN THE LEG:-
- Muscular branches to
- Tibialis posterior
- Flexor Digitorum longus
- Flexor Hallucis longus
AT THE ANKLE/FOOT:-
Medial plantar nerve:-
- Innervates abductor hallucis, flexor digitorum brevis ,flexor hallucis brevis, and first lumbrical
- Supplies medial 3.5 digits
Lateral plantar nerve:-
- Innervates the remaining intrinsic foot muscles
- Supplies the lateral 1.5 digits
- Medial calcaneal branches :-sensory innervation to the heel
ETIOLOGY
- Anatomical/structural causes:-
- Ganglion cysts, Lipoma, Varicose veins
- Medial malleolus or Talus fracture
- Tenosynovitis of the posterior tibial tendon
BIOMECHANICAL ABNORMALITIES
- Pars planus
SYSTEMIC CONDITIONS
- Diabetes Mellitus
- Inflammatory arthritis
CLINICAL FEATURES
- Burning or sharp pain along the medial ankle ,heel and sole of the foot
- Tingling, numbness or pins and needles sensation
- Intrinsic foot muscle weakness(Rare)
- Swelling near the medial malleolus(if inflammatory cause)
CLINICAL SIGNS
- Tinel’s sign-Tapping over the tarsal tunnel reproduces pain or tingling in the distribution of the tibial nerve
- Sensory loss:-Reduced sensation over the plantar surface of the foot
- Positive dorsiflexion-eversion test:-Stretching of the nerve[by dorsiflexing and everting the foot] can provoke symptoms
- Muscle wasting:-Late stage or chronic cases may show wasting of small foot muscles.
INVESTIGATIONS
IMAGING STUDIES
MRI–
- Gold standard to see soft tissue causes including ganglion cysts, tenosynovitis ,or muscle hypertrophy
ULTRASOUND
- Cost effective
- Can detect cysts, varicosities or tendon pathology compressing the nerve
X-RAY
- Helps to identify bone abnormalities, spurs or fractures that might contribute to compression
DIAGNOSTIC INJECTIONS
- Local anesthetic injection into the tarsal tunnel can cause temporary relief of symptoms supporting the diagnosis of tarsal tunnel syndrome
ELECTROPHYSIOLOGICAL STUDIES
- Nerve conduction studies:-
- Delayed conduction across the tarsal tunnel suggests compression
ELECTROMYOGRAPHY-
- Assesses muscle response and helps detect denervation in intrinsic foot muscles
- distal motor latencies of 7.0 msec or more
- prolonged sensory latencies of more than 2.3 msec
- decreased amplitude of motor action potentials of
-abductor hallucis
-or abductor digiti minimi
MANAGEMENT
NON OPEARATIVE MANAGEMENT-
Activity Modification-
- Avoid prolonged standing, walking or high impacted activities
- Adequate rest to reduce inflammation and nerve irritation
- Footwear Modifications-
- Use well-cushioned ,supportive shoes
Physical Therapy-
- Stretching and strengthening exercises for the posterior tibial tendon and intrinsic foot muscles
- Ultrasound therapy may also help to reduce soft tissue tension
Anti- inflammatory Measures-
- NSAIDS to reduce pain and inflammation
- Ice pack application
- Corticosteroid injections
- Weight Management
SURGICAL MANAGEMENT
INDICATIONS-
- after 3-6 months of failed conservative management
- Compressive mass identified
- Positive EMG
- Reproducible physical findings
TARSAL TUNNEL RELEASE
- Extend the incisions from 1 cm plantar to the navicular tuberosity in a proximal direction, bisecting the area between the medial malleolus and the medial aspect of the tuberosity of the calcaneus, ending 1cm anterior to the achilles tendon
- Dissect through the subcutaneous tissue carefully ,preserving the saphenous vein and nerve
- Retract the soft tissues to expose the flexor retinaculum
- Release of the flexor retinaculum by incising along its length to decompress the tarsal tunnel
- The tibial nerve and its branches are gently dissected free from surrounding structures
- Any fibrous band, ganglia, varicosities pr space occupying lesions are released or excised
- Hemostasis achieved and wound closed in layers
POST OPERATIVE CARE
- Immobilisation in a splint for 1-2 weeks
- Gradual weight bearing and physical therapy
- Monitor for complications like infection or nerve injury

Leave a Reply