Courtesy: Lyndon Mason FRCSOrth, Liverpool Foot and Ankle, UK
Overview
-
Talar fractures are uncommon injuries
-
There are no studies higher than Level III evidence
-
The majority of available literature consists of Level IV and Level V studies
-
Current management principles are therefore based largely on accepted clinical wisdom
Accepted Principles (“Accepted Wisdom”)
Management of talar fractures is guided by three core objectives:
-
Maintain blood supply
-
Correct deformity
-
Achieve active fracture union
Despite optimal management, complications such as:
-
Avascular necrosis (AVN)
-
Post-traumatic arthritis
remain common.
Deformity and Injury Pattern
-
Most talar fractures are the result of high-energy trauma
-
Associated deformity often involves:
-
Subtalar joint
-
Tibiotalar joint
-
Talonavicular joint
-
-
Severity of deformity correlates strongly with complications
Classification of Talar Fractures
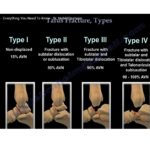
Hawkins Classification (Talar Neck Fractures)
-
Type I:
Talar neck fracture without displacement -
Type II:
Talar neck fracture with subtalar dislocation -
Type III:
Talar neck fracture with subtalar and tibiotalar dislocations -
Type IV:
Talar neck fracture with subtalar, tibiotalar, and talonavicular dislocations
Increasing Hawkins grade is associated with increasing risk of AVN.
Talar Body Fracture Classification
-
Compression fracture
-
Coronal shear fracture
-
Sagittal shear fracture
-
Fracture involving the posterior tubercle
-
Fracture involving the lateral tubercle
-
Crush fracture
Surgical Approaches
Anterolateral / Lateral Approach
-
Relatively less disruption of remaining blood supply
-
Provides better visualization of:
-
Talar neck
-
Talar body
-
-
Allows access to most talar fractures
Key Surgical Principle
-
Avoid medial approaches where possible, as they may further compromise vascularity
Fixation (“Metal Work”)
-
Screw fixation is the most common method
-
Posterior-to-anterior screw direction provides superior compression
-
Use small-footprint screws to minimize cartilage damage
-
Avoid passing screws through the flexor hallucis longus (FHL) groove
-
Limited biomechanical evidence exists to guide optimal fixation strategy
Subtalar Dislocation – Key Considerations
-
Often associated with high-energy talar neck or body fractures
-
Urgent reduction is required to:
-
Restore alignment
-
Protect soft tissues
-
Improve chances of revascularization
-
Complications
-
Overall incidence of:
-
Avascular necrosis
-
Post-traumatic osteoarthritis
-
-
Approximately 30–40%
Risk Factors for Complications
-
High-energy injury mechanisms
-
Higher Hawkins fracture types
-
Use of combined surgical approaches
-
Not significantly related to fixation strategy
Results and Fixation Techniques
-
Successful internal fixation has been reported using:
-
Two Steinmann pins
-
Passed proximally across:
-
Navicular
-
Talar head
-
Fracture site
-
Talar body
-
-
-
Maintains:
-
Neck length
-
Alignment
-
Stability during healing
-
Does Avascular Necrosis Matter?
-
In one series:
-
71.4% (10 of 14) developed talar body AVN
-
However, secondary surgery was required in only 30% (3 of 10)
-
? Presence of AVN does not always correlate with poor clinical outcome
Hawkins Sign
Definition
-
A subchondral radiolucent band in the talar dome
-
Indicates preserved talar vascularity
Characteristics
-
Appears on anteroposterior radiographs
-
Rarely visible on lateral views
-
Seen between 6 and 9 weeks post-injury
Clinical Significance
-
Absence of Hawkins sign strongly suggests AVN
-
Presence reliably excludes AVN
Diagnostic Performance
-
Sensitivity: 100%
-
Specificity: 57.7%
Summary
-
Talar fractures are rare but high-risk injuries
-
Management is guided by accepted principles:
-
Maintain blood supply
-
Correct deformity
-
Promote active union
-
-
Lateral / anterolateral approaches provide access to most talar fractures
-
Avoid medial approaches when possible
-
Bridge plating and AP screws help maintain talar neck length
-
AVN rates related to Hawkins classification have evolved with modern management
-
Presence of AVN does not always mandate further surgery
Key Take-Home Messages
-
Perfect reduction matters more than fixation choice
-
Blood supply preservation is paramount
-
Radiographic follow-up for Hawkins sign is essential
-
Complications are common but not always clinically catastrophic


Leave a Reply