Courtesy: Dr. João Espregueira Mendes (Portugal) and ASPETAR
Surgical Management of Articular Cartilage Lesions
Introduction
Articular cartilage injuries are an important cause of:
- Knee pain
- Swelling
- Functional limitation
- Early osteoarthritis
These lesions are especially significant in:
- Athletes
- Young active individuals
- Patients involved in pivoting sports
High-demand sports such as football and other pivoting activities are associated with an increased risk of osteoarthritis following cartilage injury.
Goals of Treatment
The primary objectives of cartilage restoration procedures are:
- Reduction of pain and swelling
- Improvement in joint function
- Prevention or delay of osteoarthritis progression
- Restoration of athletic performance
- Return to sports at the same competitive level
For elite athletes, return to sport is often the most important outcome measure.
Surgical Treatment Options
The major surgical procedures for cartilage restoration include:
- Microfracture
- Mosaicplasty / OATS
- Autologous Chondrocyte Implantation (ACI/MACI)
- Osteochondral Allograft Transplantation
Evidence and Current Controversies
Current evidence does not clearly demonstrate superiority of one cartilage restoration technique over another for:
- Large lesions
- Weight-bearing defects
However, important differences exist regarding:
- Return to sports
- Recovery time
- Durability of repair tissue
Return to Sports After Cartilage Procedures
Mosaicplasty / OATS
- Fastest return to sports
- Preferred for high-demand athletes
Microfracture
- Moderate return-to-sport rates
- Commonly used for smaller lesions
ACI / MACI
- Slowest return to sports
- Longer rehabilitation period
Microfracture
Principle
Microfracture involves:
- Penetration of subchondral bone
This allows:
- Marrow-derived stem cells
- Growth factors
- Blood clot formation
to fill the cartilage defect.
Advantages
- Simple technique
- Cost-effective
- Single-stage procedure
- Useful for small lesions (<1.5 cm²)
Disadvantages
- Produces fibrocartilage rather than true hyaline cartilage
- Inferior long-term durability
- Outcomes may deteriorate over time
- Less favorable for elite athletes
Clinical Role
Microfracture is most suitable for:
- Small contained lesions
- Low-demand patients
- Early focal cartilage injuries
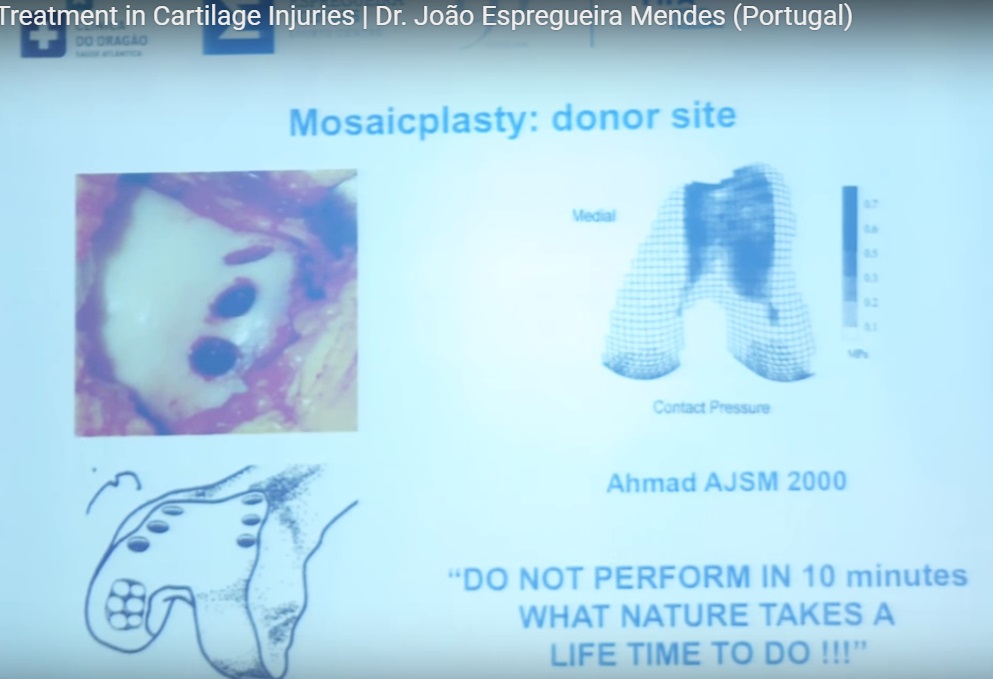
Mosaicplasty / OATS (Osteochondral Autograft Transfer)
Principle
Healthy osteochondral plugs are harvested from:
- Non-weight-bearing regions of the knee
and transplanted into the cartilage defect.
Advantages
- Restores hyaline cartilage
- Single-stage procedure
- Faster recovery and return to sports
- Addresses associated subchondral bone defects
Important Clinical Pearl
Mosaicplasty is often considered the:
- Best surgical option for athletes requiring early return to sports
Disadvantages
The major limitation is:
- Donor-site morbidity
This may lead to symptoms at the graft harvest site.
ACI and MACI
Definitions
ACI
Autologous Chondrocyte Implantation
MACI
Matrix-Induced Autologous Chondrocyte Implantation
Principle
These procedures involve:
- Harvesting chondrocytes
- Laboratory cell expansion
- Reimplantation into the cartilage defect
Advantages
- Useful for larger cartilage defects
- Potential for hyaline-like cartilage repair
Disadvantages
- Two-stage procedure
- Expensive
- Prolonged rehabilitation
- Slower return to sports
- Regulatory and logistical challenges
Clinical Outcomes
Current evidence suggests:
- No clear superiority over microfracture at medium-term follow-up
- Return-to-sport rates often below 70%
Osteochondral Allograft Transplantation
Indications
Allografts are typically used for:
- Large osteochondral defects
- Revision cartilage procedures
- Extensive subchondral bone loss
Limitations
- Limited graft availability
- Cost
- Risk of graft incorporation failure
These are generally not first-line options in routine cases.
Factors Affecting Outcomes
Several variables influence the success of cartilage restoration procedures.
Lesion Factors
- Size
- Depth
- Location
- Containment
Patient Factors
- Age
- Activity level
- Alignment
- Associated instability
Return to Sports
Overall return-to-sport rates are approximately:
- 73%
However, only about:
- 68%
return to the same preinjury competitive level.
This is an important counseling point for elite athletes.
Role of Biologics
Emerging biological adjuncts include:
- Stem cells
- Scaffolds
- Growth factors
At present, there is:
- No strong evidence proving superiority over standard techniques
Novel Osteochondral Graft Sources
Upper Tibiofibular Joint Grafts
A newer concept involves harvesting osteochondral grafts from the:
- Upper tibiofibular joint
Advantages
- Reduced donor-site morbidity
- Larger graft availability (up to approximately 5 cm²)
- Similar cartilage characteristics to femoral condyle cartilage
Limitations
- Requires advanced anatomical expertise
- Risk of injury to the common peroneal nerve
Key Concept
This technique aims to provide:
- “Mosaicplasty without donor-site morbidity”
Alignment Correction
Critical Surgical Principle
Malalignment must always be addressed during cartilage restoration surgery.
Failure to correct alignment may lead to:
- Graft overload
- Persistent symptoms
- Procedure failure
Athletes and Alignment
In athletes:
- Overcorrection should generally be avoided
- Neutral alignment is preferred
Rehabilitation
Rehabilitation is essential for successful cartilage restoration outcomes.
Key principles include:
- Early controlled motion
- Protected weight-bearing
- Gradual progression of activity
Return-to-sport timing depends on:
- Lesion size
- Procedure type
- Graft stability
- Defect location
Complications
Potential complications include:
- Graft failure
- Incomplete healing
- Persistent pain
- Donor-site morbidity
- Arthrofibrosis
- Progression to osteoarthritis
Key Clinical Pearls
- Cartilage lesions are strongly associated with early osteoarthritis.
- No single cartilage restoration technique is clearly superior in all situations.
- Mosaicplasty offers the fastest return to sports.
- Microfracture is best suited for smaller lesions.
- ACI/MACI is useful for larger defects but requires prolonged rehabilitation.
- Malalignment must always be corrected.
- Return to elite-level sports remains challenging after cartilage restoration surgery.
Final Take-Home Message
Articular cartilage restoration is a rapidly evolving field in sports medicine and joint preservation surgery.
Successful outcomes depend on:
- Proper patient selection
- Accurate lesion assessment
- Appropriate surgical technique
- Correction of associated pathology
- Structured rehabilitation
The ideal procedure should be individualized based on:
- Lesion characteristics
- Patient age
- Activity demands
- Long-term functional goals.

Leave a Reply