Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Overview
- Selection of the surgical approach for acetabular fractures depends on several factors:
- Location of the fracture within the acetabulum
- Type and pattern of the fracture
- Complexity and displacement of fracture fragments
- Proper choice of approach allows adequate exposure for reduction and fixation while minimizing complications.
Fractures Commonly Managed with a Posterior Approach
Posterior surgical exposure is typically used for fractures involving the posterior structures of the acetabulum.
Indications
- Posterior wall fractures
- Posterior column fractures
- Combined posterior wall and posterior column fractures
- Posterior wall fractures associated with transverse fracture patterns
- Selected transverse fractures when the fracture line is located low in the acetabulum
Fractures Commonly Managed with an Anterior Approach
Anterior surgical exposure allows access to fractures involving the anterior acetabular structures.
Indications
- Anterior wall fractures
- Anterior column fractures
- Associated anterior column with posterior hemi-transverse fractures
- Both column fractures
- High transverse fractures
Management of Transverse Fractures
- High transverse fractures are usually approached through an anterior approach.
- Low transverse fractures may be treated using a posterior approach depending on fracture configuration.
Combined Approaches
Certain complex fracture patterns require exposure from both sides of the acetabulum.
Indications
- T-shaped acetabular fractures
- Complex fracture patterns involving both anterior and posterior components
These fractures often require both anterior and posterior surgical approaches to achieve complete reduction.
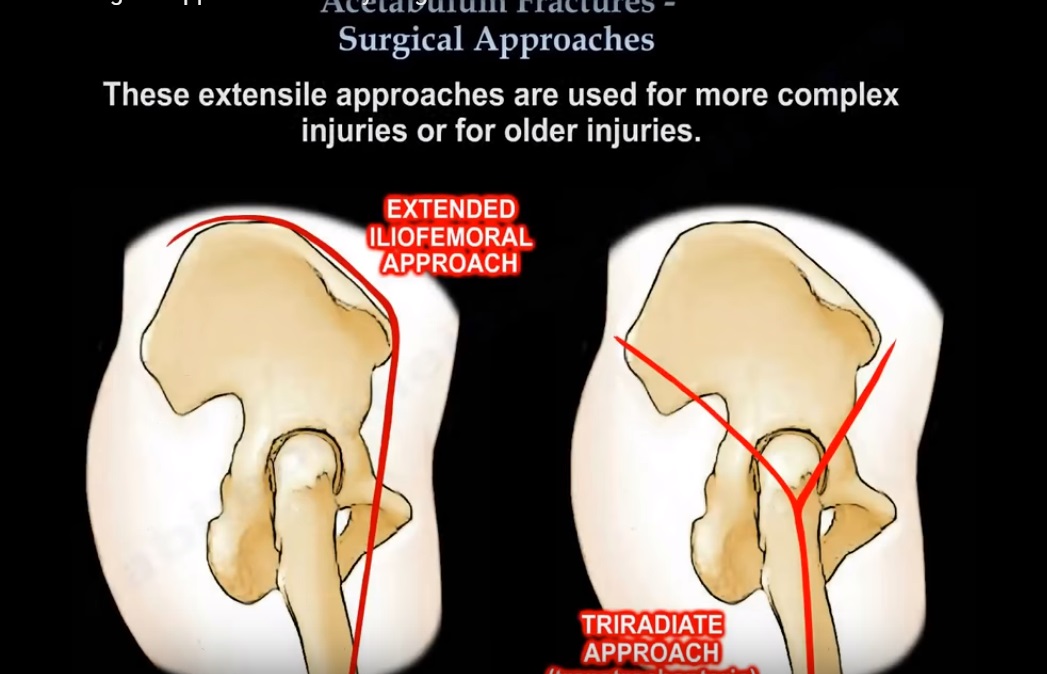
Extended Surgical Approaches
Extended approaches provide wider exposure of the acetabulum for highly complex injuries.
Types of Extended Approaches
- Extended iliofemoral approach
- Triradiate trans-trochanteric approach
Indications
- Severe or complex acetabular injuries
- Fractures requiring extensive visualization of both columns and the acetabular dome
Potential Complications
- Risk of gluteal muscle necrosis due to disruption of blood supply
- Increased risk of heterotopic ossification
In these procedures, the gluteus medius and gluteus minimus muscles may remain attached mainly through the pedicle of the superior gluteal vessels.
Heterotopic Ossification in Extended Approaches
Extended surgical exposure carries a higher risk of abnormal bone formation in soft tissues.
Prevention Strategies
- Administration of low-dose radiation therapy within seventy two hours after surgery
- Use of indomethacin therapy for approximately six weeks
These measures may reduce the severity of heterotopic ossification, although complete prevention is not always possible.
Preference for Dual Approaches
Many surgeons prefer performing separate anterior and posterior approaches instead of a single extended approach.
Reasons
- Reduced soft tissue damage
- Lower risk of heterotopic ossification
- Improved control of individual fracture components
Anterior Approach to the Acetabulum
This approach provides access to anterior column structures and pelvic brim.
Fractures Accessible Through This Approach
- Anterior column fractures
- Anterior wall fractures
- Both column fractures
- High transverse fractures
- Associated anterior column with posterior hemi-transverse fractures
Surgical Windows in the Anterior Approach
The anterior approach typically involves three surgical windows.
Medial Window
- Contains the spermatic cord in males or round ligament in females
- The ilioinguinal nerve is present in this region
- Inadequate repair of abdominal wall muscles may lead to postoperative hernia
Middle Window
- Contains the external iliac vessels
- May also contain the vascular structure known as the corona mortis
Lateral Window
- Contains the iliopsoas muscle
- Contains the femoral nerve
- Contains the lateral femoral cutaneous nerve of the thigh
These structures must be carefully protected during dissection.
Iliopectineal Fascia
- The iliopectineal fascia lies between the middle and lateral surgical windows.
- Incising this fascia along the pelvic brim allows communication between the true pelvis and the false pelvis.
- This step improves visualization and access for fracture reduction.
Important Risks in the Anterior Approach
Lateral Femoral Cutaneous Nerve Injury
- Injury may lead to sensory disturbance over the lateral thigh.
Abdominal Wall Hernia
- May occur if the abdominal wall muscles are not adequately repaired during closure.
Corona Mortis Injury
The corona mortis is a vascular connection between branches of the internal iliac system and the external iliac or inferior epigastric vessels.
Characteristics
- Located on the superior pubic ramus
- Typically found approximately three to seven centimeters from the pubic symphysis
- The location and size of this vessel vary among individuals
Clinical Significance
- Injury to this vessel during pelvic trauma or surgery can cause significant bleeding that may be difficult to control.
Posterior Approach to the Acetabulum
Posterior exposure is useful for fractures involving the posterior acetabular structures.
Indications
- Posterior wall fractures
- Posterior column fractures
- Fractures with significant posterior wall displacement
- Selected transverse fracture patterns
Surgical Considerations
- Posterior exposure can be extended by combining it with anterior incisions or trochanteric osteotomy.
Sliding Trochanteric Osteotomy
- Improves visualization of the acetabular dome and superior region of the joint.
Complications Associated with Posterior Approaches
Sciatic Nerve Injury
- The sciatic nerve must be carefully protected during dissection and retraction.
Limited Access to Anterior Structures
- Anteriorly displaced fractures may not be adequately visualized through this approach.
Disruption of Femoral Head Blood Supply
- Excessive capsular damage may compromise the vascular supply to the femoral head.
To reduce this risk, a cuff of capsular tissue approximately one centimeter wide should be preserved.
Protection of the Sciatic Nerve During Posterior Exposure
- The knee should remain flexed during the procedure to reduce tension on the sciatic nerve.
- This is particularly important when applying traction.
Retractor Placement
- A retractor placed in the greater sciatic notch can assist exposure.
- The obturator internus muscle acts as a protective layer between the retractor and the sciatic nerve.
Anatomical Relationships
- The sciatic nerve lies posterior to the obturator internus muscle.
- The nerve lies anterior to the piriformis muscle.
Safe Screw Placement in the Acetabulum
- Certain areas of the acetabulum are considered danger zones for screw placement.
- Screws placed in these areas may penetrate the hip joint.
Precautions
- Use multiple fluoroscopic views during surgery.
- Direct visualization of the joint may be used to confirm screw placement.
Fixation of Posterior Wall Fractures
- Buttress plates or hook plates are commonly used to support comminuted posterior wall fragments.
- Marginal impaction may require elevation of the impacted fragment followed by bone grafting.
Soft Tissue Injury Associated with Acetabular Trauma
Morel-Lavallée Lesion
- A Morel-Lavallée lesion is a closed soft tissue degloving injury.
- It occurs when shear forces separate the skin and subcutaneous tissues from the underlying fascia.
Clinical Features
- Commonly occurs around the pelvis and greater trochanter region.
- May develop after high-energy trauma.
Surgical Consideration
- These lesions can increase the risk of infection because up to thirty percent of operative sites may be colonized by bacteria at the time of surgery.
Leave a Reply