Courtesy: Prof Nabil Ebraheim, Unviersity of Toledo, Ohio, USA
Subscapularis Tendon Tear
Introduction
The subscapularis tendon is an essential component of the rotator cuff and plays a major role in:
- Internal rotation of the shoulder
- Anterior shoulder stability
Subscapularis tears are commonly:
- Underdiagnosed
- Missed clinically
especially when associated with:
- Biceps tendon instability
- Combined rotator cuff pathology
Early recognition is important to preserve shoulder function and prevent progression of tendon degeneration.
Relevant Anatomy
Subscapularis Muscle
The subscapularis is:
- The largest and strongest muscle of the rotator cuff
It originates from the:
- Subscapular fossa of the scapula
and inserts onto the:
- Lesser tuberosity of the humerus
The tendon contributes approximately:
- 50% of total rotator cuff strength
Other Rotator Cuff Insertions
The remaining rotator cuff tendons insert onto the:
- Greater tuberosity
These include:
- Supraspinatus
- Infraspinatus
- Teres minor
Relationship to the Biceps Tendon
The long head of the biceps tendon runs within the:
- Bicipital groove
and is stabilized by:
- Transverse humeral ligament
- Subscapularis tendon
The subscapularis acts as an important:
- Dynamic stabilizer of the biceps tendon
Function
Primary Function
The primary action of the subscapularis is:
- Internal rotation of the shoulder
Secondary Functions
Additional functions include:
- Adduction
- Anterior stabilization of the glenohumeral joint
Importantly, the subscapularis is not a primary abductor of the shoulder.
Nerve Supply
The subscapularis is supplied by:
- Upper subscapular nerve
- Lower subscapular nerve
Both arise from the:
- Posterior cord of the brachial plexus
Etiology
Traumatic Causes
Traumatic tears may occur after:
- Anterior shoulder dislocation
- Fall on an outstretched arm
- Forced external rotation injury
Degenerative Causes
Degenerative tears commonly occur in:
- Chronic rotator cuff disease
Iatrogenic Causes
Subscapularis injury may occur following:
- Shoulder arthroplasty
- Other shoulder surgery
Associated Bony Injury
Tears may be associated with:
- Lesser tuberosity avulsion fractures
Association with Biceps Pathology
There is a strong relationship between:
- Subscapularis tears
- Biceps tendon instability
Approximately:
- 80–90% of biceps instability cases
have associated subscapularis pathology.
Types of Tears
Subscapularis injuries may occur as:
- Isolated tears
- Combined tears
Combined tears often involve:
- Supraspinatus
- Infraspinatus
Pathophysiology
Tearing of the subscapularis disrupts the:
- Anterior force couple of the shoulder
This can result in:
- Anterior shoulder dysfunction
- Biceps tendon instability
- Weakness of internal rotation
Clinical Presentation
Pain
Patients typically present with:
- Anterior shoulder pain
Weakness
Weakness is most notable during:
- Internal rotation
Range of Motion Changes
Patients may demonstrate:
- Increased passive external rotation
due to loss of anterior restraint.
Acute vs Chronic Presentation
Tears may present as:
- Acute traumatic injuries
- Chronic degenerative tears
Chronic tears are commonly missed.
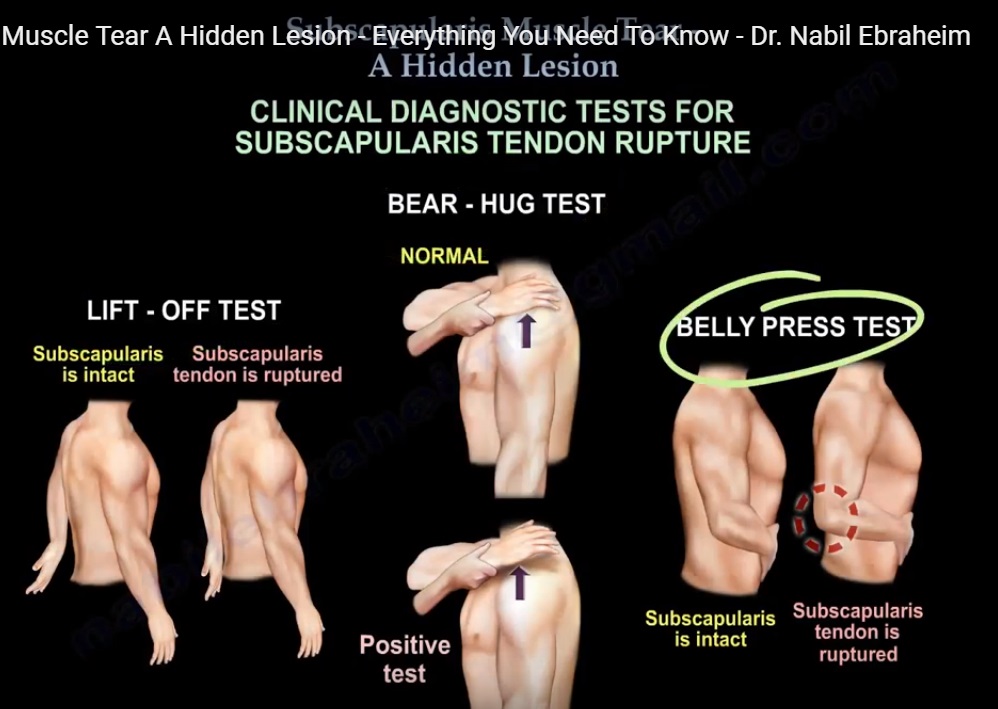
Physical Examination
Lift-Off Test
Technique
- Patient places hand behind the back
- Attempts to lift hand away from the body
Positive Test
Inability to lift the hand suggests:
- Subscapularis tear
Belly Press Test
Technique
- Patient presses the abdomen while keeping elbow forward
Positive Test
A positive test occurs when:
- The elbow drifts backward
indicating internal rotation weakness.
Bear Hug Test
Technique
- Hand placed on opposite shoulder
- Examiner attempts to lift the hand away
Positive Test
Weakness or inability to resist indicates:
- Subscapularis dysfunction
Imaging
Ultrasound
Ultrasound is useful for:
- Initial screening
- Dynamic evaluation
MRI
MRI is considered the:
- Gold standard imaging modality
MRI findings include:
- Tendon detachment from lesser tuberosity
- Tendon retraction
- Muscle atrophy
Muscle atrophy is an important prognostic factor.
Special Imaging and Arthroscopic Signs
Comma Sign
The comma sign represents avulsed fibers of the:
- Superior glenohumeral ligament
- Coracohumeral ligament
This finding helps identify:
- Retracted subscapularis tears during arthroscopy
Special Clinical Scenario
After shoulder arthroplasty, patients with:
- Increased passive external rotation
- Persistent weakness
- Normal radiographs
should be evaluated for:
- Subscapularis failure
using ultrasound or MRI.
Associated Conditions
Reverse Hill-Sachs Lesion
A reverse Hill-Sachs lesion is:
- An impaction fracture of the anteromedial humeral head
typically associated with:
- Posterior shoulder dislocation
Modified McLaughlin Procedure
Defects involving less than 50% of the humeral head may be treated using:
- Subscapularis tendon transfer
- Lesser tuberosity transfer
This is commonly known as the:
- Modified McLaughlin procedure
Management
Acute Complete Tears
Acute full-thickness tears are usually treated with:
- Surgical repair
Repair may be:
- Arthroscopic
- Open
Associated Biceps Procedures
When biceps instability is present, treatment may include:
- Biceps tenodesis
- Biceps tenotomy
Chronic Tears
Chronic tears may become:
- Retracted
- Atrophied
- Irreparable
Tendon Transfer Procedures
In irreparable cases, treatment options include:
- Pectoralis major tendon transfer
This helps restore:
- Anterior shoulder force balance
and improves:
- Pain
- Function
Massive Irreparable Posterosuperior Tears
Young patients with massive posterosuperior cuff tears may undergo:
- Latissimus dorsi tendon transfer
An intact subscapularis is essential before considering this procedure.
Postoperative Rehabilitation
Postoperative management includes:
- Protection of the repair
- Gradual rehabilitation
Early excessive external rotation should be avoided to protect healing tissue.
Complications
Potential complications include:
- Persistent weakness
- Re-tear
- Shoulder stiffness
- Residual instability
- Progressive rotator cuff arthropathy
Differential Diagnosis
Conditions that may mimic subscapularis pathology include:
- Biceps Tendon Instability
- Rotator Cuff Tear
- Shoulder impingement syndrome
- Adhesive capsulitis
- Cervical radiculopathy
Key Clinical Pearls
- Subscapularis tears are among the most commonly missed rotator cuff injuries.
- Anterior shoulder pain with internal rotation weakness should raise suspicion.
- Biceps tendon instability is strongly associated.
- Lift-off, belly press, and bear hug tests are important examination maneuvers.
- MRI findings must always be correlated clinically.
- Chronic tears may become irreparable because of retraction and muscle atrophy.
Final Take-Home Message
Subscapularis tendon tears are important but frequently underdiagnosed shoulder injuries that significantly affect internal rotation strength and anterior shoulder stability.
Patients commonly present with:
- Anterior shoulder pain
- Internal rotation weakness
- Biceps tendon instability
Careful clinical examination combined with MRI evaluation is essential for diagnosis.
Early surgical repair provides the best outcomes, while chronic irreparable tears may require tendon transfer procedures to restore shoulder function.

Leave a Reply