Courtesy: Dr Anil Oommen, Dr Ashok Shyam, Ortho TV
Overview
- Spinopelvic mobility has gained increasing attention in recent years in the field of total hip arthroplasty.
- Many cases of postoperative dislocation are now understood to be related to overlooked factors involving the interaction between the spine and the pelvis.
- Understanding this relationship is important for proper acetabular cup positioning and for reducing complications after surgery.
Relationship Between Spine and Pelvis
- Movement of the spine and pelvis is interconnected during posture changes.
- When a person moves from sitting to standing, both the spine and pelvis adjust simultaneously.
- In a normal standing posture, the pelvis usually tilts anteriorly.
- In a sitting posture, the pelvis typically tilts posteriorly.
- The degree of change between sitting and standing varies between individuals and is considered patient-specific.
- These changes are reflected in the presence or absence of lumbar lordosis on radiographic images.
- The functional orientation of the pelvis differs from one person to another due to differences in pelvic tilt.
Clinical Importance
- Certain patients are more prone to problems related to spinopelvic mobility.
- Individuals with ankylosing spondylitis often have a fused spine and reduced pelvic motion.
- In such cases, improper acetabular cup orientation can lead to instability or dislocation after total hip arthroplasty.
- Careful evaluation of spinal stiffness and spinopelvic mobility is therefore essential before surgery.
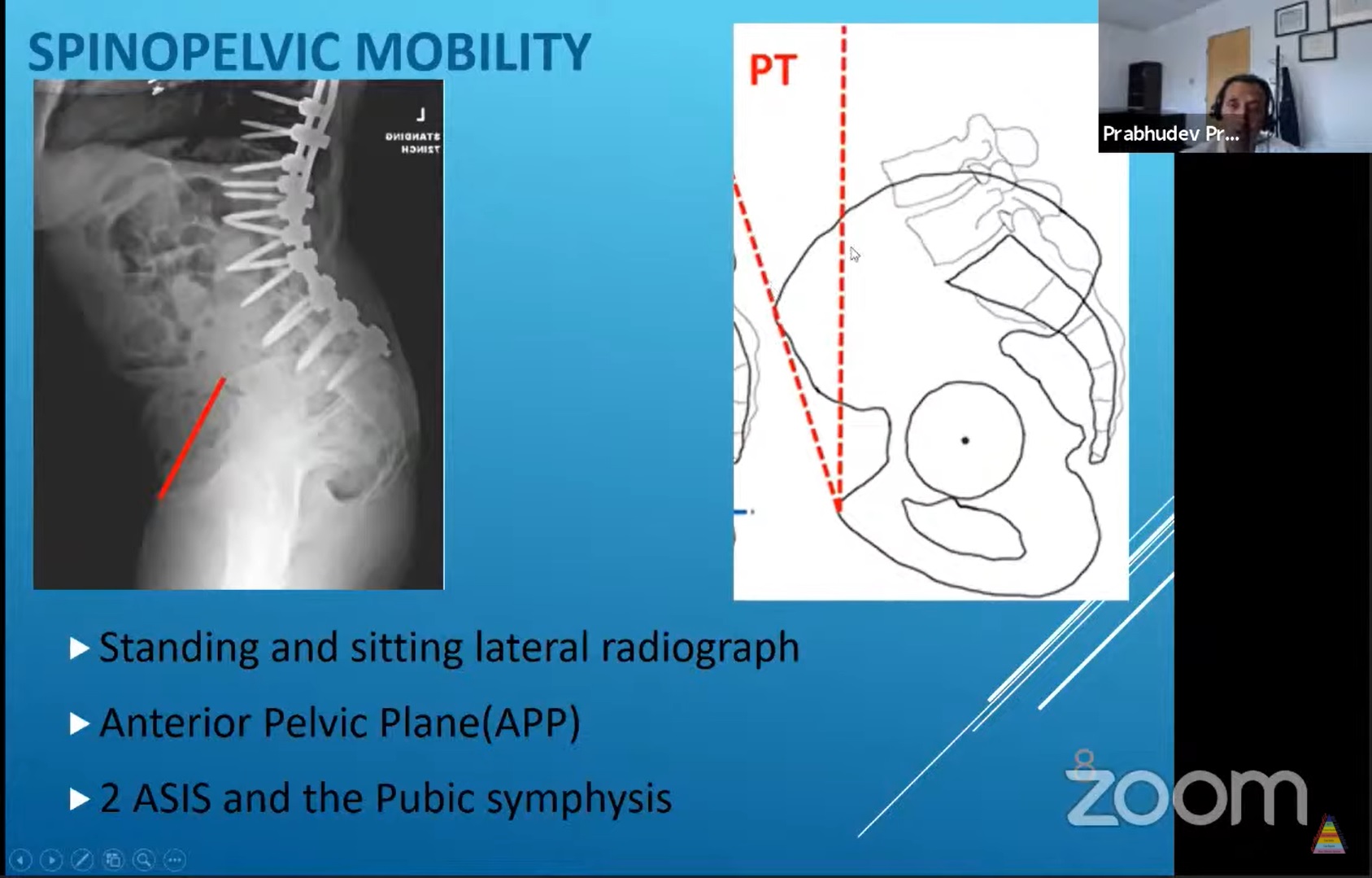
Radiographic Assessment
- Preoperative evaluation should include lateral radiographs of the spine and pelvis in both sitting and standing positions.
- These images help determine the degree of pelvic tilt change during posture transition.
- Several spinopelvic parameters can be assessed, including:
- Lumbar lordosis
- Pelvic tilt
- Sacral slope
- Pelvic inclination
- Among these, sacral slope is commonly used as a simple and reliable indicator.
Sacral Slope and Normal Motion
- In normal individuals, the sacral slope changes approximately ten to thirty degrees when moving from sitting to standing.
- This change reflects normal spinopelvic mobility.
- Limited variation indicates reduced mobility or spinal stiffness.
Influence on Acetabular Cup Orientation
- Pelvic tilt significantly affects the functional orientation of the acetabular cup.
- A change in pelvic tilt alters both cup inclination and anteversion.
- Approximately every ten degree change in pelvic tilt results in:
- About seven degree change in anteversion
- About three degree change in inclination
- In the sitting position, the pelvis rotates posteriorly, increasing functional anteversion.
- In the standing position, the pelvis rotates anteriorly, producing relative retroversion.
Risk of Impingement and Dislocation
- Incorrect cup orientation combined with abnormal spinopelvic motion can lead to:
- Anterior or posterior impingement
- Eccentric wear of the prosthesis
- Hip dislocation
- Adjustments in cup placement may be required based on individual spinopelvic mechanics.
Patterns of Spinopelvic Mobility
Stuck Sitting Pattern
- Sacral slope remains less than approximately thirty degrees in both sitting and standing positions.
- Associated with reduced lumbar lordosis.
- Common in patients with ankylosing spondylitis.
- The pelvis remains relatively posteriorly tilted with minimal movement.
Stuck Standing Pattern
- Sacral slope remains greater than approximately thirty degrees with little change between positions.
- Persistent lumbar lordosis is present.
- Often seen in patients with degenerative spine disease or spinal instrumentation.
Clinical Implications of Mobility Patterns
Stuck Standing Pattern
- Limited spinal flexion may lead to anterior impingement.
- Increased risk of posterior hip dislocation.
- Slightly increased acetabular anteversion may help reduce this risk.
Stuck Sitting Pattern
- Limited spinal extension causes posterior impingement.
- Increased risk of anterior dislocation.
- Reduced acetabular anteversion may be recommended.
Special Considerations in Ankylosing Spondylitis
- The spine and pelvis may function as a rigid unit with minimal mobility.
- Spinopelvic parameters often remain unchanged even after hip replacement.
- Many patients demonstrate a persistent stuck sitting pattern.
- Careful adjustment of acetabular anteversion is important to prevent instability.
Implant Strategy
- Dual mobility implants are often recommended in patients with abnormal spinopelvic mechanics.
- These implants can reduce the risk of postoperative dislocation in high-risk cases.
Practical Surgical Considerations
- Spinopelvic mobility should be assessed before performing total hip arthroplasty.
- Preoperative standing and sitting lateral radiographs of the spine and pelvis are essential.
- Acetabular cup positioning should be adjusted according to individual spinopelvic characteristics.
- When advanced technology is unavailable, careful use of anatomical landmarks and surgical technique remains important.
Key Takeaways
- Spinopelvic mobility plays a critical role in the stability of total hip arthroplasty.
- Patient-specific evaluation helps guide appropriate acetabular cup positioning.
- Recognition of abnormal mobility patterns can help prevent impingement and dislocation.
- Thorough preoperative assessment and thoughtful implant strategy improve surgical outcomes.


Leave a Reply