Courtesy: Sally Hobson, Hull Royal Infirmary, UK
Definition
-
Slipped capital femoral epiphysis is a Salter–Harris Type I injury occurring through the hypertrophic zone of the proximal femoral growth plate.
-
The femoral head remains within the acetabulum, while the femoral neck and shaft displace superolaterally and externally rotate relative to the epiphysis.
Epidemiology
-
Commonly occurs between 9 and 13 years of age.
-
Presentation tends to occur earlier in girls than in boys.
-
Bilateral involvement occurs in approximately 30 percent of cases.
Risk Factors
-
Occurs during the pre-pubertal growth spurt.
-
Increased shear forces across the physis.
-
Obesity, although not present in all cases.
-
Endocrine and metabolic disorders, including:
-
Hypothyroidism
-
Cushing syndrome
-
Rickets
-
-
Connective tissue disorders such as Marfan syndrome.
-
History of irradiation or chemotherapy.
-
Down syndrome.
Clinical Presentation
-
Presentation patterns:
-
Acute on chronic: approximately 50 percent
-
Acute: approximately 20 percent
-
Chronic: approximately 30 percent
-
-
Symptoms include:
-
Pain in the hip, thigh, or knee
-
Irritable hip
-
-
Clinical signs include:
-
Limb shortening and external rotation, more pronounced in severe slips
-
Restricted internal rotation of the hip
-
Obligatory external rotation during hip flexion
-
Investigations
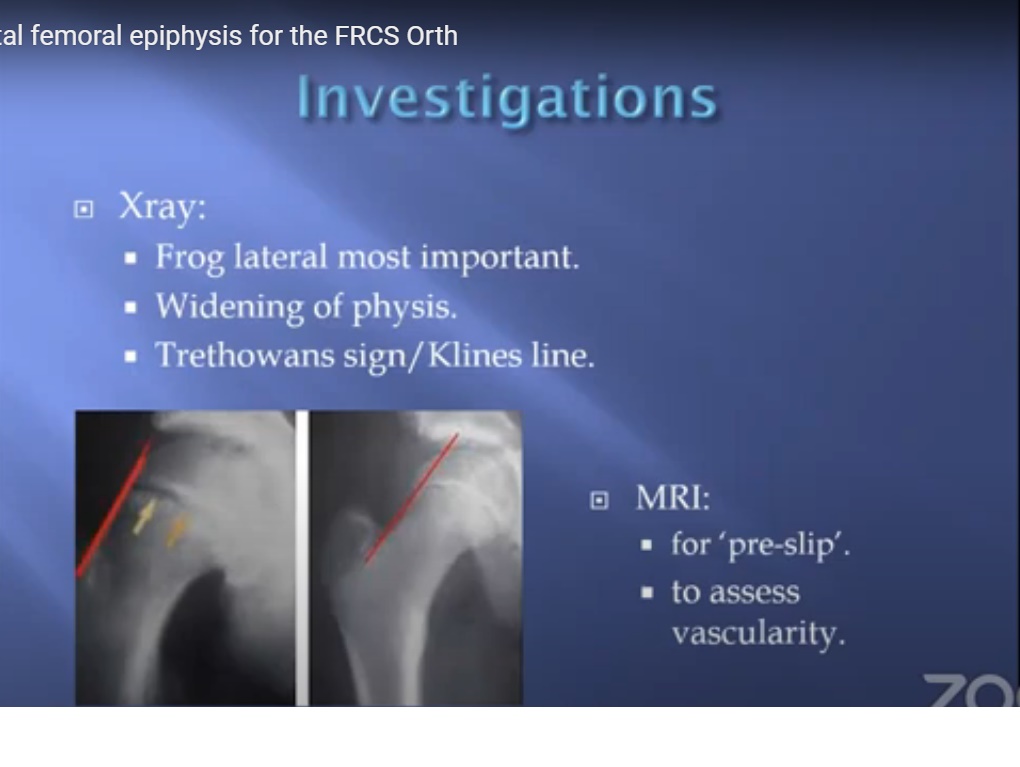
Radiography
-
Frog-leg lateral view of the hip is the most important radiographic view.
-
Findings may include:
-
Widening of the physis
-
Posterior and inferior displacement of the femoral head
-
Trethowan Sign (Klein Line)
-
A line drawn along the superior border of the femoral neck on the anteroposterior view should intersect the femoral head.
-
In slipped capital femoral epiphysis, the line passes superior to the femoral head.
Magnetic Resonance Imaging
-
Useful for diagnosing pre-slip or early disease.
-
Helps assess the vascularity of the femoral head, particularly in unstable slips.
Classification
Loder Classification
-
Stable slipped capital femoral epiphysis: patient is able to bear weight, with or without crutches.
-
Unstable slipped capital femoral epiphysis: patient is unable to bear weight.
-
Stability is the most important predictor of avascular necrosis.
Southwick Angle Classification
-
Quantitative assessment of slip severity using lateral radiographs.
-
A slip angle greater than 60 degrees is considered severe.
Treatment Principles
-
Strict bed rest until surgical intervention.
-
Prompt surgical stabilization is required to prevent further slippage.
Surgical Management
Gold Standard Treatment
-
In situ fixation using a single cannulated screw.
-
Key technical considerations:
-
Entry point should be anterior on the femoral neck.
-
Fluoroscopic screening through the full range of hip motion to ensure no joint penetration.
-
The screw is intended to remain permanent.
-
Management of Severe Slips
-
Options include:
-
In situ pinning
-
Gentle, controlled reduction when deemed safe
-
Open reduction techniques, including:
-
Modified Dunn osteotomy
-
Surgical hip dislocation, when indicated
-
-
-
These procedures carry a high risk of avascular necrosis.
-
National and international guidelines emphasize caution due to this risk.
Prophylactic Fixation of the Contralateral Hip
-
Considered in patients at high risk for bilateral disease.
-
Decision is based on:
-
Presence of endocrine or metabolic abnormalities
-
Younger age at presentation
-
Patient compliance
-
Increased posterior sloping angle
-
Complications
Chondrolysis
-
Often related to:
-
Intra-articular screw penetration
-
Guidewire advancement into the joint
-
-
Prevention requires meticulous intraoperative imaging.
Avascular Necrosis
-
Most commonly occurs in severe and unstable slips.
-
Typically leads to significant pain, joint destruction, and poor outcomes.
Femoroacetabular Impingement
-
Cam-type impingement may develop following in situ fixation.
-
Results in:
-
Externally rotated gait
-
Limb shortening
-
Progressive hip dysfunction
-
Late Screw-Related Complications
-
Late screw penetration due to collapse or avascular necrosis.
-
Growth of the femoral neck away from the screw in younger patients.


Leave a Reply