Courtesy: Dr. Sudhir Warrier, Dr Ashok Shyam, Ortho TV
Introduction
Injuries to the proximal interphalangeal joint are among the most common injuries of the hand. They are frequently encountered in sports such as cricket, where the finger is struck directly by a ball. Despite their frequency, these injuries are often missed or underestimated, which can lead to long-term stiffness and functional impairment.
Missed diagnoses usually occur because of:
-
Inadequate history taking
-
Incomplete clinical examination
-
Improper or insufficient radiographic evaluation
Common Mechanisms of Injury
Typical causes include:
-
Direct impact from a ball
-
Twisting injuries to the finger
-
Road traffic accidents, particularly motorcycle injuries
Clinical Evaluation
Accurate diagnosis requires a detailed history and focused examination of the injured finger.
Common Clinical Findings
Patients may present with:
-
Swelling around the proximal interphalangeal joint
-
Bruising of the finger
-
Pain and localized tenderness
-
Reduced finger flexion or extension
A careful comparison with the opposite finger is often helpful.
Radiological Evaluation
Plain radiography is the most important investigation for diagnosing proximal interphalangeal joint injuries.
Recommended Radiographic Views
Radiographs should be taken of the specific injured finger, rather than the entire hand.
Required views include:
-
Anteroposterior view
-
True lateral view
-
Oblique views
Multiple lateral views may sometimes be necessary to identify subtle subluxations or fractures.
Computed tomography is rarely required when properly positioned radiographs are available.
Proximal Interphalangeal Joint Fracture–Dislocations
Fracture-dislocations of the proximal interphalangeal joint represent complex injuries involving both bone and ligament structures.
Factors Determining Treatment
Management decisions depend primarily on:
-
Time elapsed since injury
-
Percentage of articular surface involvement
-
Stability of the joint
Management of Acute Injuries
When the Articular Surface Is Intact
Closed reduction is often sufficient.
Reduction Principles
-
Gentle traction is applied to the finger.
-
The joint is reduced by correcting the deformity.
Most proximal interphalangeal fracture-dislocations are stable when the joint is placed in flexion.
Immobilization
-
The finger is immobilized in flexion for approximately two weeks.
Healing Considerations
During healing, the volar plate tends to heal in slight flexion.
This often results in:
-
Mild flexion contracture of the proximal interphalangeal joint.
Follow-Up Assessment
At approximately six weeks, stability should be reassessed using flexion–extension radiographs.
Management of Flexion Contracture
Flexion contracture is a common consequence of proximal interphalangeal joint injuries.
Treatment Options
Management typically involves the use of a Capener spring splint.
Splinting protocol:
-
Initially used intermittently during the day
-
Later continued as night splinting
This gradually restores extension over time.
Traction Techniques
Certain injuries can be managed using traction methods.
Methods
Options include:
-
Finger traction
-
Finger strapping techniques
-
Nail traction in selected cases
Duration
Traction is generally maintained for two to three weeks, depending on joint stability.
Extensor Block Pinning
Indications
This technique is used when:
-
Closed reduction cannot be maintained
-
The fracture-dislocation remains unstable
Technique
-
Closed reduction is performed.
-
A Kirschner wire is inserted as an extensor block to prevent dorsal displacement of the middle phalanx.
This maintains joint alignment during healing.
Delayed Presentation (Two to Three Weeks After Injury)
When treatment is delayed, closed reduction may no longer be possible.
Management Option
Ligamentotaxis using Kirschner wire traction can be employed.
Principle
External traction gradually restores:
-
Joint alignment
-
Articular congruity
Even delayed cases can achieve good functional outcomes with this method.
Late Presentation (Six Weeks or More)
Chronic injuries require reconstructive procedures.
Surgical Options
Possible treatments include:
-
Volar plate arthroplasty
-
Hemi-hamate arthroplasty
-
Open reduction and internal fixation
Alternative Approach
External distractor fixation may still be useful.
Traction may allow:
-
The volar fragment to be pulled into position
-
Restoration of articular congruity.
Very Late Presentation (Months After Injury)
If the fracture has united in an abnormal position:
Surgical Management
Treatment may involve:
-
Open reduction with corrective osteotomy
Fixation methods include:
-
Small screws
-
Extensor block pinning if instability persists.
Blunt Proximal Interphalangeal Joint Injuries
Some injuries occur without visible fractures on radiographs.
These injuries are frequently underestimated.
Typical Presentation
Patients may have:
-
Swelling of the joint
-
Preserved finger flexion
-
Later development of extension weakness.
Risk
Untreated injuries often lead to progressive flexion contracture.
Management of Blunt Injuries
Once fracture is excluded, treatment includes:
-
Ice therapy
-
Nonsteroidal anti-inflammatory medication
-
Immobilization using a dorsal gutter splint in extension for approximately two weeks
-
Active distal interphalangeal joint exercises during splinting.
Low-Cost Splint Option
A simple splint can be fabricated using:
-
A cut twenty milliliter syringe
-
Soft padding
-
Adhesive tape for fixation
This provides a practical and inexpensive immobilization method.
Assessing Contracture Reversibility
A useful clinical test is the passive extension test.
Interpretation
-
Painful passive extension suggests the contracture is reversible and likely to respond to splinting.
-
Fixed contracture may require surgical treatment.
Surgical Management of Severe Contractures
Procedure
A volar surgical approach is used.
Structures that may require release include:
-
Flexor tendon sheath
-
Volar capsule
-
Contracted soft tissues.
Postoperative Care
Successful recovery requires:
-
Early finger mobilization
-
Continued use of a Capener splint for three to six months.
Proximal Interphalangeal Joint Dislocations
Clinical Features
Dislocations are usually obvious.
Typical findings include:
-
Severe pain
-
Visible finger deformity
-
Markedly restricted motion.
Diagnosis
Radiographs are necessary to exclude associated fractures.
Treatment of Dislocations
Closed reduction is usually adequate.
Post-Reduction Care
-
Avoid hyperextension for approximately two weeks.
-
Encourage early controlled mobilization to prevent stiffness.
Key Principles in Managing Proximal Interphalangeal Joint Injuries
Radiological Assessment
-
Always obtain a true lateral radiograph.
-
Flexion–extension radiographs may help assess joint stability.
Stability Characteristics
-
Many proximal interphalangeal fracture-dislocations are stable when the joint is flexed.
Traction Techniques
Common methods include:
-
Nail traction
-
Finger strapping
-
Extensor block pinning
-
External distractor fixation.
Common Sequela
Flexion contracture is a frequent complication.
Management typically involves Capener spring splinting.
Key Take-Home Messages
-
Always obtain multiple radiographic views of the injured finger.
-
A true lateral radiograph is essential for diagnosis.
-
Proximal interphalangeal fracture-dislocations are usually stable in flexion.
-
Early injuries can often be treated non-operatively.
-
Delayed injuries may require:
-
Traction techniques
-
External fixation
-
Reconstructive procedures
-
-
Blunt injuries without fracture still require early treatment to prevent contracture.
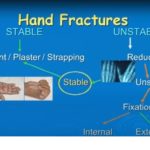
Hand Fractures: General Management Principles
A Common Clinical Problem
Hand fractures are frequently undertreated or improperly immobilized.
Poor management can lead to:
-
Finger stiffness
-
Rotational deformity
-
Permanent functional impairment.
Basic Principles of Treatment
Management of hand fractures follows four essential steps:
-
Assess the injury
-
Reduce the fracture
-
Stabilize the fracture
-
Mobilize the hand appropriately
Importance of Proper Radiographs
Standard hand radiographs may be inadequate.
Essential imaging includes:
-
True lateral radiograph of the injured finger
-
Properly positioned views for accurate fracture assessment.
Practical Description of Hand Fractures
A useful clinical description should include:
-
Bone involved
-
Location within the bone
-
Whether the fracture is intra-articular or extra-articular
-
Degree of displacement
-
Stability of the fracture
-
Presence of deformity.
Example Description
Closed undisplaced oblique fracture of the shaft of the proximal phalanx of the index finger.
Criteria for Stability
A fracture is considered stable when:
-
At least fifty percent active range of motion is present in adjacent joints
-
No dynamic deformity occurs during motion
-
No rotational deformity is present.
Stable fractures can usually be managed conservatively.
Conservative Treatment
Buddy Taping
-
Micropore tape is preferred.
-
Elastic adhesive bandage should be avoided.
Application Principles
-
Avoid covering joint creases.
-
Allow joint movement to prevent stiffness.
Functional Position of the Hand
During immobilization, the hand should be maintained in the functional position.
Recommended alignment:
-
Wrist: approximately thirty degrees of extension
-
Metacarpophalangeal joints: forty five to sixty degrees of flexion
-
Interphalangeal joints: full extension
-
Thumb: opposition
Failure to maintain this position can lead to hand stiffness and poor functional outcome.
Principles of Kirschner Wire Fixation
Indications
Kirschner wire fixation is used when:
-
The fracture is unstable
-
Closed reduction cannot maintain alignment.
Technical Considerations
-
Use the minimum number of wires necessary.
-
Avoid injury to tendons and soft tissues.
-
Avoid distraction across the fracture.
Technical Details of Wire Placement
-
The wire should cross the far cortex for stability.
-
Short trocar-tip wires are often preferred.
-
The cutting action occurs along the sharp edges of the wire rather than the tip.
Management of Intra-Articular Fractures
Treatment options include:
-
Screw fixation
-
Kirschner wire fixation
-
Plate fixation in complex fractures.
Treatment Goal
The objective is to restore joint congruity and enable early mobilization.
Volar Lip Fractures of the Proximal Interphalangeal Joint
A key radiological sign is the “V sign” seen on the lateral radiograph.
Significance
This indicates dorsal subluxation of the middle phalanx.
Treatment Options
-
Closed reduction
-
Extension-block splinting
-
Nail traction in unstable cases.
Management of Late Cases
Untreated injuries may require hemi-hamate arthroplasty to reconstruct the joint surface.
Rehabilitation
Rehabilitation is essential for successful outcomes.
Key components include:
-
Early controlled motion
-
Proper splinting
-
Structured physiotherapy.
Surgical treatment alone will not restore function without rehabilitation.
Core Principle of Hand Fracture Management
The hand must always be immobilized in the functional position:
-
Wrist in extension
-
Metacarpophalangeal joints flexed
-
Interphalangeal joints extended
-
Thumb in opposition
Failure to maintain this position can result in severe stiffness and poor hand function.


Leave a Reply