Introduction
-
Scapular Dyskinesis (SD) refers to an alteration in normal scapular motion and positioning.
-
Leads to disruption of the scapulohumeral rhythm (SHR).
-
It is not a diagnosis or isolated injury, but a functional impairment.
-
Commonly occurs secondary to shoulder girdle pathology.
Prevalence in Athletes
-
61% in overhead athletes (throwers, swimmers, tennis players)
-
33% in non-overhead athletes
Purpose of This Review
-
Understand scapular biomechanics and anatomy
-
Recognize clinical features of SD
-
Learn evaluation and diagnostic methods
-
Review treatment strategies
-
Highlight sport-specific implications and management
Periscapular Anatomy & Biomechanics
Scapular Anatomy
-
Large, flat, triangular bone
-
Connects the axial skeleton to the arm via:
-
Acromioclavicular (AC) joint
-
Sternoclavicular (SC) joint
-
-
Minimal bony stability
-
Highly dependent on muscular control
Primary Stabilizing Muscles
-
Major muscles
-
Trapezius (upper, middle, lower)
-
Serratus anterior
-
Rhomboids
-
-
Scapulothoracic bursae
-
Infraserratus
-
Supraserratus
-
Scapulotrapezial
-
Potential sources of pain and snapping
-
Functional Role
-
Provides a stable base for humeral motion
-
Essential for:
-
Arm elevation
-
Rotation
-
Force transfer during overhead sports
-
Etiology of Scapular Dyskinesis
| Category | Mechanism | Examples |
|---|---|---|
| Primary SD | Muscle or neurological dysfunction | Muscle fatigue, imbalance |
| Neurological | Nerve injury | Long thoracic, spinal accessory, dorsal scapular nerves |
| Bony | Structural abnormalities | Scapular fractures, clavicle malunion, thoracic kyphosis |
| Joint Pathology | Shoulder girdle joint disease | AC/SC arthrosis, instability |
| Soft Tissue | Tightness or inflexibility | Pectoralis minor, posterior capsule |
| Associated Pathology | Secondary to shoulder injury | Labral tears, rotator cuff disease |
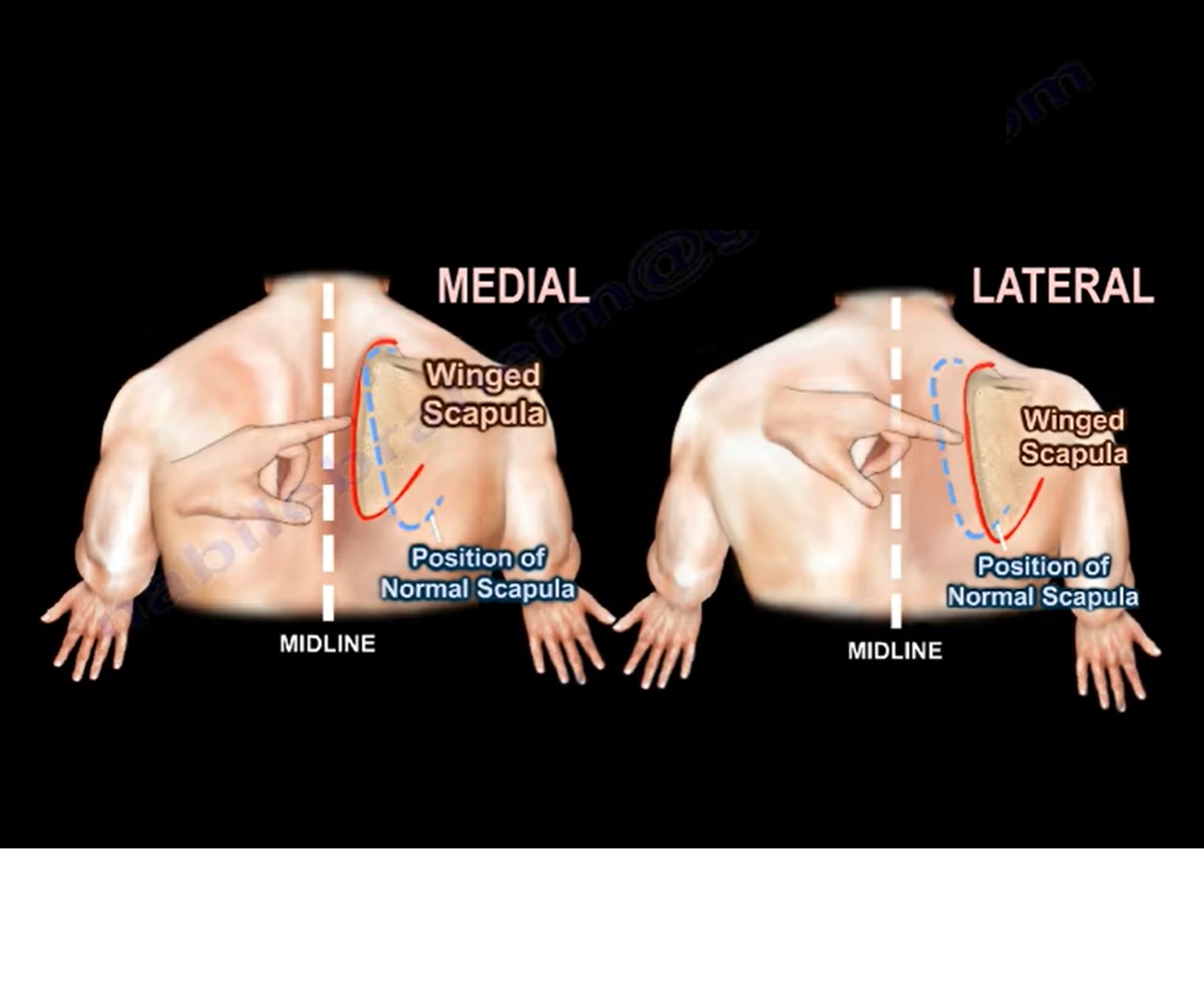
Neurological Causes of Scapular Winging
-
Medial winging
-
Long thoracic nerve injury
-
Serratus anterior weakness
-
-
Lateral winging
-
Spinal accessory nerve (trapezius)
-
Dorsal scapular nerve (rhomboids)
-
Kibler Classification of Scapular Dyskinesis
| Type | Key Feature | Abnormality |
|---|---|---|
| Type I | Inferomedial border prominence | Abnormal rotation about transverse axis |
| Type II | Entire medial border prominence | Abnormal rotation about vertical axis |
| Type III | Superomedial border prominence | Superior scapular translation |
| Type IV | Normal | Normal scapular motion |
SICK Scapula Syndrome
| Component | Description |
|---|---|
| S | Scapular malposition |
| I | Inferomedial border prominence |
| C | Coracoid pain and malposition |
| K | Kinesis (movement) dysfunction |
Clinical Assessment of Scapular Dyskinesis
History
-
Often gradual and insidious onset
-
Common complaints in overhead athletes:
-
“Dead arm” sensation
-
Loss of control and strength
-
Early fatigue
-
-
May coexist with or cause shoulder impingement
-
Periscapular pain:
-
Posterior border
-
Anterior pain near the coracoid
-
Physical Examination
Visual Observation
-
Observe for:
-
Asymmetry
-
Winging
-
Dysrhythmia during arm elevation/lowering
-
-
Perform Scapular Dyskinesis Test (SDT) with and without weights
Resting Position Evaluation
-
Arms relaxed at sides
-
Assess:
-
Vertical scapular asymmetry
-
Lateral displacement from midline
-
Scapular abduction angle (goniometer)
-
Dynamic Motion
-
Forward flexion and lowering
-
Look for:
-
Border prominence
-
Irregular or jerky motion
-
Muscle Strength Testing
-
Upper trapezius – shoulder shrug
-
Middle trapezius – prone, arm at 90°, resist downward force
-
Lower trapezius – prone, arm abducted 120°
-
Rhomboids – modified Kendall test
-
Serratus anterior
-
Wall push-ups
-
Look for medial border winging
-
Special Tests
-
Scapular Assistance Test
-
Examiner assists upward rotation/posterior tilt
-
Positive if pain decreases or motion improves
-
-
Scapular Retraction Test
-
Scapula stabilized during impingement testing
-
Positive if pain reduces or strength improves
-
Additional Findings
-
Local tenderness (borders, coracoid, AC joint)
-
Crepitus ? possible snapping scapula syndrome
Imaging & Diagnostic Studies
| Modality | Purpose | Indications |
|---|---|---|
| X-ray | Bony assessment | Alignment, fractures |
| MRI shoulder | Soft tissue evaluation | Rotator cuff, labrum |
| MRI scapula | Scapulothoracic pathology | Bursitis, snapping scapula |
| CT scan | Detailed bony anatomy | Deformity, fractures |
| Cervical MRI | Neurological cause | Suspected radiculopathy |
| EMG / NCV | Nerve & muscle function | Long thoracic or spinal accessory nerve injury |
Treatment of Scapular Dyskinesis
Non-Operative (Mainstay)
-
Focused physical therapy
-
Restore flexibility first
-
Activate scapular stabilizers
-
-
Muscle training
-
Serratus anterior
-
Lower trapezius
-
-
Exercise progression
-
Begin below shoulder level
-
Progress to kinetic chain and sport-specific drills
-
Rehabilitation Timeline
-
Typically 2–12 weeks
-
Scapular-focused programs show better outcomes than generalized rehab
Surgical Management
-
Rarely required
-
Reserved for:
-
Snapping scapula
-
Refractory scapulothoracic bursitis
-
Structural abnormalities
-
-
Arthroscopic excision and correction
Sport-Specific Considerations
Baseball (Throwers & Pitchers)
-
High-velocity overhead throwing stresses the shoulder
-
Deceleration phase causes:
-
Posterior capsular tightness
-
GIRD (Glenohumeral Internal Rotation Deficit)
-
-
SD associated with:
-
Increased scapular internal rotation
-
Reduced shoulder rotation velocity
-
Reduced scapular motion
-
-
Risk factors:
-
Low external rotation strength
-
Reduced internal rotation
-
-
Rehabilitation
-
Effective when addressing posterior tightness
-
Early intervention reduces injury risk
-
Swimming
-
Up to 90% of propulsion from upper limbs
-
Annual shoulder pain prevalence: 23–38%
-
“Swimmer’s shoulder” includes:
-
Impingement
-
Rotator cuff tendinopathy
-
Instability
-
SD
-
-
SD prevalence increases with fatigue:
-
30% pre-training
-
70% mid-training
-
80% post-training
-
-
More common in:
-
Long-distance swimmers
-
Athletes with >4 years of training
-
Male swimmers
-
-
Conservative management leads to faster return to sport
Tennis
-
Repetitive high-velocity serving stresses the shoulder
-
SD disrupts the kinetic chain
-
Findings in tennis players:
-
Reduced subacromial space
-
Decreased racket velocity
-
-
Common associated injuries:
-
GIRD
-
SLAP tears
-
Shoulder impingement
-
-
Treatment
-
Physiotherapy focusing on:
-
Scapular control
-
Core strength
-
Posterior capsule stretching
-
-
Key Take-Home Messages
-
Scapular dyskinesis is a functional abnormality, not a standalone injury
-
Strongly associated with multiple shoulder pathologies
-
Athletes with shoulder pain must be assessed for SD
-
Most cases respond well to scapula-based rehabilitation
-
Underlying pathology should be treated alongside SD to prevent recurrence

Leave a Reply