Courtesy: Vaikunthan Rajarathnam, Hand Surgeon
Scapholunate Ligament Injury
Introduction
- The scapholunate ligament is the primary stabilizer between the scaphoid and lunate
- Maintains normal carpal alignment and wrist biomechanics
- The dorsal component is the strongest and most functionally important portion
Injury can lead to:
- Wrist instability
- Weakness
- Progressive arthritis
- Carpal collapse
Anatomy
Components of the Ligament
- Dorsal portion
- Proximal membranous portion
- Volar portion
Important Anatomical Facts
Dorsal Portion
- Thickest and strongest component
- Main stabilizing structure
- Approximately 2 mm thick
Volar Portion
- Thin and relatively weak
Normal Scapholunate Interval
- Approximately 5 mm
Epidemiology
- Common cause of wrist instability
- Approximately 5% of wrist sprains involve the scapholunate ligament
Injury severity ranges from:
- Mild attenuation
- Partial tear
- Complete rupture
Grading of Injury
Mild Injury
- Ligament stretching
- No major separation
Moderate Injury
- Partial tear
- Increased scapholunate gap
Severe Injury
- Complete rupture with instability
Important point:
- Gap >2 mm suggests significant injury
- Gap may increase with loading or stress views
Arthroscopic Classification
Grade 1
- Attenuation
- <2 mm separation
Grade 2
- Increased separation
- No gross instability
Grade 3
- Gap >2 mm
Grade 4
- Arthroscope can pass through scapholunate interval
Classification Based on Site of Rupture
Type 1
- Rupture at scaphoid attachment
- Most common
Type 2
- Rupture at lunate attachment
Type 3
- Mid-substance tear
Type 4
- Partial tear with attenuation
Important Surgical Point
- Types 1 and 2 are most suitable for direct repair
Pathomechanics and Carpal Instability
Normal Tendencies
- Scaphoid tends to flex
- Lunate tends to extend
After Ligament Injury
- Scaphoid flexes volarly
- Lunate extends dorsally
- Scapholunate angle increases
- Capitate migrates into widened interval
Results:
- Carpal instability
- Altered wrist biomechanics
- Progressive degeneration
Clinical Features
Patients may present with:
- Wrist pain
- Weakness
- Reduced grip strength
- Mechanical symptoms
Watson Test
Positive Test
- Pain or clunk during radial deviation
Suggests:
- Scapholunate instability
Imaging
X-rays
May show:
- Widened scapholunate gap
- Dynamic instability on stress or clenched-fist views
MRI
- Increased signal at ligament site
- Assesses soft tissue injury
Wrist Arthroscopy
- Gold standard for diagnosis and grading
Non-Surgical Management
Indications
- Acute injuries
- Mild stable injuries
Treatment
- Splint immobilization
- Rehabilitation
- Strengthening of wrist stabilizers
Good functional recovery possible in stable injuries.
Important Considerations in Management
Assess:
- Integrity of ligament
- Possibility of primary repair
- Alignment of scaphoid and lunate
- Reducibility of deformity
- Articular cartilage status
Surgical Management
Acute Injuries (Within 4–6 Weeks)
Treatment
- Direct ligament repair
- Temporary K-wire fixation
Purpose of fixation:
- Protect repair during healing
Subacute Injuries (6 Weeks–4 Months)
- Direct repair becomes more difficult
- Reconstruction or augmented stabilization may be needed
Chronic Dynamic Instability
Ligament Reconstruction
Often uses:
- Flexor carpi radialis tendon graft
Technique:
- Bone tunnels created in:
- Scaphoid
- Lunate
- Temporary fixation often added
Advanced Disease
Chronic instability may progress to:
- Degenerative arthritis
- SLAC wrist (Scapholunate Advanced Collapse)
Treatment depends on extent of arthritis.
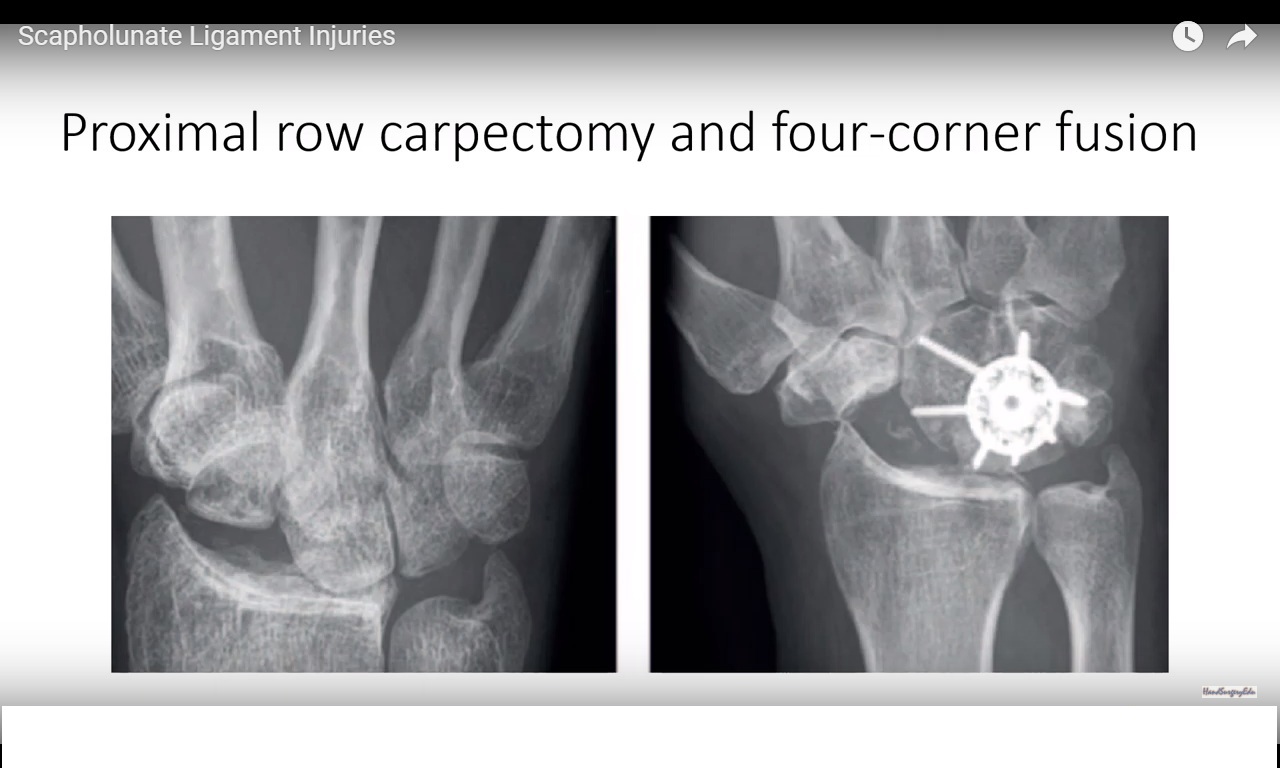
Salvage Procedures
Proximal Row Carpectomy (PRC)
Procedure
Removal of:
- Scaphoid
- Lunate
- Triquetrum
Capitate articulates directly with radius.
Advantages
- Pain relief
- Preserves partial wrist motion
Requirement:
- Intact radiocapitate cartilage
Four-Corner Fusion
Procedure
- Scaphoid excision
- Fusion of midcarpal joints
Provides:
- Stability
- Acceptable functional motion
Indication:
- Midcarpal arthritis
Key Clinical Pearls
- Dorsal component is the strongest and most important stabilizer
- Gap >2 mm suggests significant injury
- Watson test helps detect instability
- Arthroscopy is the gold standard diagnostic tool
- Untreated injuries lead to progressive carpal instability and arthritis
- Acute injuries may be repaired directly
- Chronic instability often requires reconstruction
- Salvage options include:
- Proximal row carpectomy
- Four-corner fusion
Leave a Reply