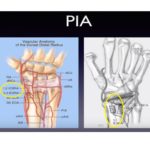
Courtesy: Gustavo Gomez Rodriguez, Buenos Aires, Argentina
Scaphoid Nonunion: Principles of Management
Overview
- Scaphoid nonunion occurs because of:
- Fragment instability
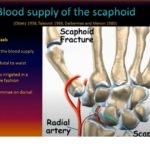
- Poor blood supply to proximal pole
- Large cartilage-covered surface
- Exposure to synovial fluid
- Successful treatment requires:
- Fracture union
- Restoration of normal scaphoid anatomy
- Correction of deformity
- Failure to restore anatomy can lead to:
- Abnormal wrist mechanics
- Progressive arthritis
- Carpal collapse
Normal Wrist Biomechanics
Under Axial Loading
- Scaphoid tends to flex
- Triquetrum tends to extend
- Distal carpal row pronates in coordinated motion
After fracture:
- Distal fragment:
- Flexes
- Pronates with distal carpal row
- Proximal fragment:
- Extends with proximal carpal row
Pathomechanics of Scaphoid Nonunion
Distal Fragment
- Flexion + pronation
- Impinges against radial styloid
Proximal Fragment
- Extends dorsally
Result:
- Increased intrascaphoid angle
- Reduced scaphoid height
- Humpback deformity
- DISI deformity
- Progressive carpal malalignment
Causes of Nonunion
- Fragment displacement
- Poor proximal pole vascularity
- Synovial fluid exposure
- Persistent instability
Degenerative Progression
Early Arthritis
- Between distal scaphoid fragment and radial styloid
Later Progression
- Midcarpal degeneration
- Advanced radiocarpal arthritis
This progression is called:
- Scaphoid Nonunion Advanced Collapse (SNAC wrist)
Evaluation
CT Scan – Most Important Investigation
CT assesses:
- Site of nonunion
- Degree of deformity
- Intrascaphoid angle
- Scaphoid height
- Bone quality
- Trabecular pattern
- Progress of healing
Goal of imaging:
- Assess both union and restoration of anatomy
Main Treatment Goals
- Achieve bony union
- Restore scaphoid length
- Restore scaphoid height
- Correct humpback deformity
- Reduce intrascaphoid angle
- Restore carpal congruity and alignment
Treatment Options
1. Fixation Alone
- Selected nonunions with:
- Good biology
- Minimal deformity
2. Nonstructural Cancellous Bone Graft
- Supports union
- Used when major deformity correction is not needed
3. Structural Corticocancellous Bone Graft
Preferred When Deformity Exists
Advantages:
- Restores scaphoid shape
- Corrects humpback deformity
- Provides mechanical support
Graft sources:
- Iliac crest
- Distal radius
Distal Radius Structural Graft Technique
Advantages:
- Same operative field
- Less donor-site morbidity
Key steps:
- Expose nonunion
- Remove sclerotic bone
- Reach healthy bleeding bone
- Correct deformity
- Pack cancellous graft
- Insert structural graft volarly
- Fix with compression screw
Importance of Deformity Correction
- Union alone is insufficient if malalignment persists
- Restoration of scaphoid height is critical
- Midcarpal congruity must be reassessed after fixation
Vascularized Bone Grafting
Indications
Used in:
- Poor biology
- Recalcitrant nonunion
- Proximal pole nonunion with vascular compromise
Common Vascularized Graft
1,2 Intercompartmental Supraretinacular Artery Graft
- Pedicled dorsal distal radius graft
Fixation:
- Screw fixation
- K-wire fixation
Role of Vascularized Grafts
Potential advantages:
- Improved biology
- Faster healing
Important point:
- Not proven superior in all studies
- Not every proximal pole nonunion requires vascularized grafting
Reserved mainly for:
- Difficult nonunions
- Revision cases
- Compromised vascularity
Follow-Up
Assess:
- Maintenance of reduction
- Scaphoid height
- Intrascaphoid angle
- Graft position
- Progress toward union
CT is particularly useful during early healing.
Practical Surgical Points
- Compression screw fixation commonly used
- Additional K-wire support may improve rotational stability
- Accurate reduction is as important as union
- Malunion can produce major functional problems
Complications
- Persistent nonunion
- Malunion
- Loss of correction
- Progressive carpal collapse
- Degenerative arthritis
- Wrist pain and stiffness
Key Exam Pearls
- Scaphoid nonunion occurs due to:
- Instability
- Poor proximal pole blood supply
- Synovial environment
- Humpback deformity:
- Increased intrascaphoid angle
- Reduced scaphoid height
- CT scan is the best investigation for:
- Planning
- Follow-up
- Structural graft preferred when deformity correction is required
- Vascularized grafts usually reserved for:
- Difficult
- Recurrent
- Biologically compromised nonunions


Leave a Reply