Courtesy: Dr Hamid R Abbasi, Dr Ashok Shyam, Ortho TV
Sacroiliac Joint Dysfunction – High-Yield Review
Introduction
Sacroiliac (SI) joint dysfunction is an important and frequently underdiagnosed cause of low back pain.
Recognition of SI joint pathology dates back to the early 1900s, yet it continues to be overlooked in many patients with persistent back pain.
Why the SI Joint Matters
Epidemiology
Important statistics include:
- Approximately 22% of low back pain originates from the SI joint
- After lumbar fusion surgery, especially at L4–L5 and L5–S1, nearly 43% of persistent pain may arise from the SI joint
Clinical Importance
Many patients labeled as having:
- Failed back surgery syndrome
may actually have unrecognized SI joint pathology.
Important Clinical Concept
“The Patient May Have Two Problems”
SI joint dysfunction commonly coexists with:
- Lumbar spine pathology
- Hip disorders
Treating only one pathology may leave the patient symptomatic and dissatisfied.
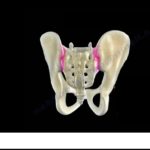
Anatomy of the Sacroiliac Joint
Unique Joint Characteristics
The SI joint is not a typical synovial joint.
It behaves more like a:
- Partially synovial
- Partially ligamentous
- Remnant-type joint
Movement
Normal SI joint movement is very limited:
- Approximately 2–4 degrees
Motion greater than this may become pathological.
Structural Components
The SI joint consists of:
- Articular portion
- Ligamentous portion
Important Anatomical Point
The SI joint often appears degenerative or arthritic on imaging even in asymptomatic individuals.
There is also significant anatomical variability.
Risk Factors for SI Joint Dysfunction
Important risk factors include:
- Female gender
- Postpartum state
- Younger age compared with typical degenerative spine patients
- Minor trauma
Postpartum women have significantly increased risk for approximately two years after delivery.
The “Chameleon Joint”
SI joint dysfunction can mimic many other disorders, including:
- L5–S1 disc herniation
- Lumbar facet pain
- Hip pathology
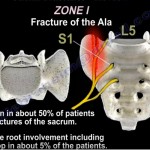
- Sacral insufficiency fracture
Any radicular pain pattern may potentially originate from the SI joint.
Clinical Diagnosis
History
Typical Pain Location
Pain is commonly localized near:
- Posterior superior iliac spine (PSIS)
Aggravating Factors
Pain may worsen with:
- Turning in bed
- Weight bearing
- Transitional movements
Fortin Finger Test
Technique
The patient points to the area of maximal pain.
Positive Test
Pain localized within approximately one inch of the SI joint is highly suggestive of SI joint pathology.
Provocation Tests
Because the SI joint is very strong and stable, provocation testing requires substantial force.
Multiple positive provocative maneuvers increase diagnostic accuracy.
Rapid SI Joint Test
Technique
- Patient places ankle over opposite knee
- Increasing downward force is applied
Positive Test
Reproduction of typical SI joint pain suggests pathology.
This is a quick and practical outpatient test.
Confirmatory Diagnosis
Diagnostic Injection – Gold Standard
Image-guided diagnostic injection remains the gold standard for confirming SI joint pain.
Important Principles
Diagnostic injection should include:
- Fluoroscopic or CT guidance
- Small volume anesthetic (<2 mL)
- Contrast confirmation
Diagnostic Criteria
Typically requires:
- Two positive injections
- At least 75% pain relief
This confirms the SI joint as the primary pain generator.
Treatments with Limited Effectiveness
Interventions with less predictable benefit include:
- Bracing
- Blind injections
- Radiofrequency ablation
Radiofrequency procedures tend to be less effective than in facet-mediated spine pain.
Evidence Supporting Surgery
Randomized controlled trials have shown:
- Conservative treatment groups often worsen over time
- Surgically treated patients demonstrate significant improvement
- Many non-operative patients eventually cross over to surgery
Careful patient selection is critical.
Surgical Management
Open SI Joint Fusion
Historically used but now largely obsolete except in trauma situations.
Disadvantages include:
- Extensive blood loss
- Larger surgical exposure
- Higher morbidity
Minimally Invasive SI Joint Fusion
Preferred Modern Technique
Most procedures now use a:
- Lateral-to-medial minimally invasive approach
Advantages
- Smaller incision
- Less tissue disruption
- Faster recovery
- Improved patient satisfaction
Important Surgical Considerations
Surgeons must avoid injury to:
- Internal pelvic structures
- Superior gluteal artery
Intraoperative Imaging
Essential imaging views include:
- True lateral view
- Inlet view
- Outlet view
These help ensure safe implant positioning.
Fixation Methods
Older Techniques
Included:
- Wedges
- Cages
These are now less commonly used.
Modern Preferred Technique
Trident Screw Technique
Technique involves:
- Initial placement of one screw
- Placement of additional screws through similar trajectory
Advantages include:
- Strong fixation
- Short operative time
- Efficient workflow
Implant Biology
Modern implants are designed for:
- Osteointegration
Surface Characteristics
Optimal pore size is approximately:
- 70–140 microns
This promotes bone ingrowth and biological fixation.
Additional bone grafting is often unnecessary.
Key Clinical Pearls
- Always consider the SI joint in persistent low back pain.
- SI joint dysfunction is especially common after lumbar fusion.
- Young females and postpartum patients are higher-risk groups.
- Atypical radicular pain patterns may originate from the SI joint.
- Diagnostic injection is the gold standard for diagnosis.
- Minimally invasive SI fusion can provide excellent outcomes in properly selected patients.
Final Take-Home Message
The sacroiliac joint is a major but frequently overlooked source of low back pain.
It is particularly important to evaluate the SI joint in patients with:
- Failed spine surgery
- Persistent unexplained back pain
- Atypical radiculopathy
- Postpartum pain syndromes
Missing SI joint pathology may leave patients symptomatic despite otherwise successful spine treatment.


Leave a Reply