Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
SACRAL FRACTURES
- The Sacrum is connected to the pelvis through Sacro-Iliac joints
- Sacrum Fractures can have neurological deficit (maybe a nerve root injury or involvement of the Cauda Equina which affects the bladder, bowel and the sexual function ) – it will decide the outcome of the patient
- If L4 and L5 nerve root are involved – Foot Drop
- Sacral nerve roots can be affected
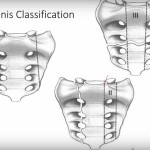
Three types of Sacral Fractures
1. Zone 1 fracture
– Alar fracture,
– Lateral to the foramen
– Most common type (50% of patient)
– L5 nerve root involvement (5% of the patient)
– Fixed percutaneously
2. Zone 2 fracture
– Foraminal fractures
– Through the foramen
– Usually stable fractures
– Can be unstable with a vertical shear force (the worst type – difficult
fracture to fix, increase the risk of fracture displacement, non-union, failure of fixation and very poor functional outcome),
– About 80 % percent of these have a sacral nerve root injury
3. Zone 3 fracture
– Sacral canal affected
– Medial to the foramen
– About 60 to 80 % have neurological deficit
– Can affect the Cauda Equina
– Two types – Longitudinal or Transverse
Transverse fracture – Mostly similar to ‘U’ type, axial loading causes transverse fracture at the weakest area located between S2 and S3
– It has two parts, part that goes with the spine and the other part goes with the pelvis
– It creates a spinal pelvic dissociation.
Clinical Presentation
– 25% have neurological injury
– Do Rectal Examination
– Do examination of S1 -S5 dermatome (the sensation around the perianal area)
Imaging
– X-Rays : Hard to see sacral fractures (AP, Lateral Sacral, Inlet and Outlet views)
– AP view: Will show disruption of the arcuate lines and involvement of the foramen
Double Shadow – Indicates transverse fractures.
– Outlet view: Shows the foramen, any vertical displacement of the fracture
– Lateral Sacral view: Shows the U-shaped fracture (similar to transverse fracture)
– CT scan in the study of choice
– MRI will show the status of the nerve root and the Cauda Equina
Treatment
– Minimally invasive sacral fractures – do progressive weight-bearing plus crutches or a walker
– Surgical fixation if the fracture is unstable, displaced or if there is neurological deficit
– Avoid over compression of fracture – may cause nerve injury
– May need to decompress the neural elements for improvement of neurological status
Fixation of Sacral Fractures
– Percutaneous Screws
– Posterior Tension Band Plating
– Compression Bar Technique
– The Triangular Fixation – the best technique, combined iliosacral and lumbo-pelvic fixation
– It has the greatest stiffness for unstable sacral fractures.


Thank you so much for sharing Thiago one !