Courtesy: Herve Ouanezar MD

Topic: Ramp Lesion Repair During ACL Reconstruction
Introduction & Acknowledgments
-
Gratitude for the invitation and acknowledgment of key mentors and groups.
-
Primary Focus: Sharing insights on ramp lesion repair in ACL injuries.
Presentation Outline
1. Definition and History
-
Isolated ACL injuries: Only 25% of cases.
-
Combined Lesions: Present in 75% of ACL cases.
-
Three Main Combined Lesions:
-
Medial meniscus ramp lesion
-
Lateral meniscus root tear
-
Anterolateral ligament/complex injury
-
-
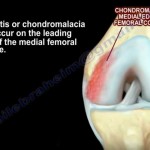
Definition of Ramp Lesion:
-
Disruption of the peripheral meniscocapsular attachment of the posterior horn of the medial meniscus.
-
Detection:
-
Often missed when probing from the front.
-
Requires a posterior approach with an arthroscope.
-
-
-
Historical Development:
-
First described by Gillquist (1983).
-
Craig Morgan (1991) introduced all-inside meniscus repair with hook sutures.
-
Recent studies from Korea focus on clinical outcomes of this repair technique.
-
2. Biomechanics of Ramp Lesions
-
Caused by:
-
Anterior-posterior translation of the tibia.
-
Internal rotation of the knee.
-
Shear forces from semimembranosus contraction.
-
-
Impact on Stability:
-
Medial meniscus acts as a secondary stabilizer.
-
Ramp lesions contribute to posterior instability.
-
3. Epidemiology
-
Prevalence:
-
Initial studies (2014): Found only 4-5% incidence.
-
Advancements in technique (2020): Found up to 20% incidence.
-
Large-Scale Studies:
-
Santi Group (3,214 patients) found 24% prevalence in primary ACL cases.
-
Revision ACL cases: 40% prevalence.
-
-
-
Key Takeaway: If the surgeon does not detect a ramp lesion, the lesion will eventually reveal itself through complications.
4. Diagnosis and Imaging
-
MRI Indicators:
-
Bone bruise on the posterior medial tibial plateau.
-
Often missed on MRI, so direct arthroscopic examination is necessary.
-
-
Systematic Arthroscopic Diagnosis (French Arthroscopic Society, 2014):
-
Probe the meniscus from the front.
-
Push the arthroscope to the posterior medial corner.
-
Open the thin layer to check for hidden lesions.
-
5. Treatment and Surgical Techniques
Should Stable Ramp Lesions Be Left Untreated?
-
Chinese Study: Suggests some stable lesions may heal spontaneously with simple debridement.
-
French Study (8-Year Follow-Up):
-
Findings:
-
33% of untreated ramp lesions resulted in complications.
-
Often led to large bucket-handle tears.
-
-
Conclusion: Ramp lesions should be repaired to prevent long-term issues.
-
Surgical Repair Techniques
-
Step-by-Step Approach:
-
Probe the meniscus.
-
Identify the lesion through posterior medial arthroscopy.
-
Use transillumination for safe incision (avoiding the saphenous nerve).
-
Refresh the tear edges with a shaver.
-
Internal rotation of the tibia helps expose the tear for repair.
-
-
Preferred Repair Method:
-
Use all-inside hook sutures for precise reattachment.
-
Non-absorbable sutures (PDS0) to prevent suture-related complications.
-
Multiple stitches improve stability (typically 2-3 per tear).
-
-
Why Not Use Suture Anchors or Fast-Fix Devices?
-
Higher risk of floating anchors (13% incidence).
-
Difficulty in closing the lesion properly.
-
Increased risk of failure when knee moves into extension.
-
6. Clinical Results
Comparison of Repair Techniques
-
Briotet Study (Lyon Group):
-
All-inside suture anchors had a 31% failure rate.
-
Hook suture technique reduced failure rate to 16%.
-
-
Santi Group (3,214 patients):
-
All-inside anchors: ~25-30% failure rate.
-
Hook sutures: Lower failure rate (15% for isolated ACL, 6.6% if combined with ALL reconstruction).
-
7. Complications & Prevention
-
Common Complications (1.5% cases):
-
Hematoma.
-
Saphenous nerve hypoesthesia.
-
-
Prevention Strategies:
-
Use transillumination before making the incision.
-
Turn off room lights to clearly visualize nerve and vessels.
-
Conclusion & Key Takeaways
-
High Incidence of Ramp Lesions:
-
24% in primary ACL injuries.
-
39% in revision ACL cases.
-
-
Systematic Arthroscopic Approach is Essential.
-
Biomechanical Importance:
-
Repairing ramp lesions restores rotational stability.
-
Reduces anterior tibial translation.
-
-
Best Surgical Practice:
-
Use hook sutures for better outcomes.
-
Combined reconstruction (e.g., ALL repair) further lowers failure rates.
-
Closing Remarks:
-
Thank you for the invitation.
-
Open discussion on ramp lesion repair.

Leave a Reply